How to plan a cardiac MRI viability protocol (part 2)
Written by:
Erik Jacobsson
This step-by-step guide is for MRI students, radiographers and technologists who wish to improve their planning skills and master the cardiac viability MRI protocol.
In this Part 2, we will follow up with tissue characterization, where we determine which damaged parts of the myocardium can recover with treatment, and which are permanently scarred.
What you will learn:
Patient and scanner setup tips.
How to perform perfusion, early, and late gadolinium enhancement.
What parameters optimize tissue characterization
Ways to avoid common contrast protocol errors.
How to identify viable vs non-viable myocardium.
Key Takeaways
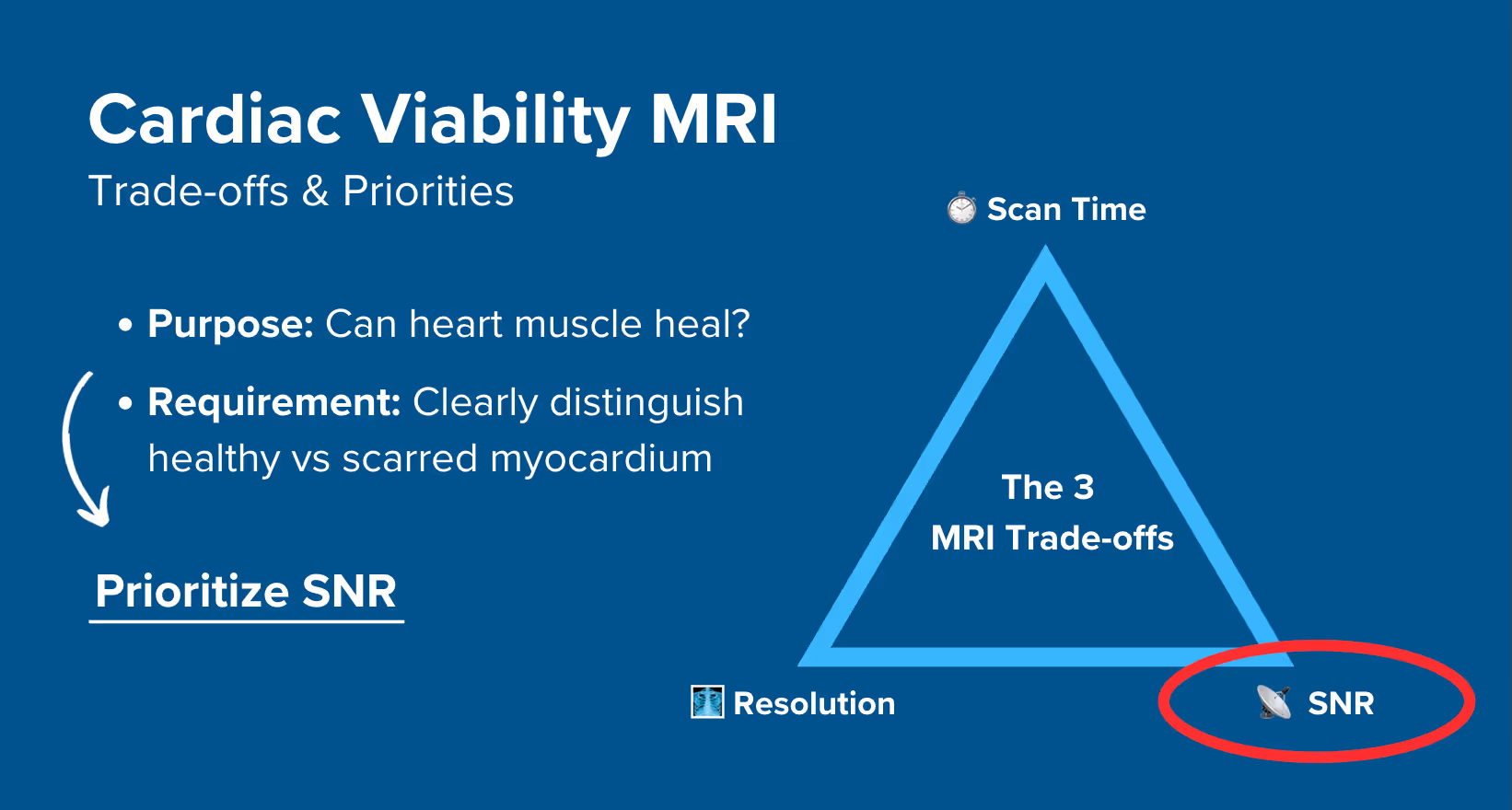
For cardiac viability MRIs, it's generally recommended to prioritize SNR, then resolution, and lastly scan time.
To identify if damaged heart muscle can still heal, we must clearly distinguish between healthy and scarred myocardium.
Strong SNR helps us differentiate bright scar tissues against dark healthy muscle.
We run 3 types of post-contrast Gradient Echo (GRE) sequences, each at specific time points and with different TI.
Sequence type
When
TI value
What it shows
Perfusion
Immediately
No inversion
Blood flow
Early Enhancement
2–4 min after contrast
Very high (440 ms)
Acute damage
Late Enhancement
10–15 min after contrast
Precise value from TI Scout (200–250 ms)
Scarred myocardium (chronic damage)
Avoid these 5 common contrast protocol mistakes.
Mistakes
Solution – How to Avoid It
Wrong TI selection
Always run a TI Scout to find the exact value that nulls healthy myocardium.
Mismatched slice positioning
Copy exact positions from earlier cine sequences to ensure comparable images.
Timing mistakes
Have all sequences ready BEFORE contrast injection. You can't pause mid-protocol.
Not enough phases
Use 60+ phases for perfusion if the heart pumps slowly to capture the full cardiac cycle.
Contrast safety issues
Always check eGFR is above 35 before injection.
Intro to Cardiac Tissue Characterization
In Part 1 of our cardiac viability protocol, we completed all function and morphology sequences. We captured the heart's pumping action with cine images and checked for structural abnormalities with black and bright blood sequences.
Now we continue with another core part of viability assessment: tissue characterization. This is where we determine which damaged heart areas can recover with treatment, and which are permanently scarred.
Distinguishing between viable and scarred myocardium is of great importance:
Viable tissue (subendocardial scars) can regain function after revascularization procedures like bypass surgery or stenting.
Non-viable tissue (transmural scars), however, won't improve. This makes aggressive treatment pointless and potentially harmful.
How to Balance the 3 Trade-offs in Cardiac Viability MRIs
In MRI, we always face a trade-off between 3 key metrics:
Scan Time: How fast a pulse sequence can be completed.
Resolution: How much detail the image can display.
SNR: How clear the image is, how much signal relative to noise.
Improving one of these metrics reduces the performance of the others. To decide what trade-offs to make, we must consider the needs of each clinical situation.
For cardiac viability MRIs:
The main goal is to clearly distinguish between scarred and healthy heart muscle.
The depth and extent of damage can be just 1–2 mm, so we also need good resolution.
Scan time matters, but we can often afford a bit more time if the patient can cooperate.
Therefore, we typically 1) prioritize SNR, 2) keep high enough resolution to assess scar depth, and 3) optimize for scan time as needed based on patient ability.
This balance ensures we clearly see bright scar tissue against the dark, viable myocardium, which is the whole point of viability imaging.
Note! Prioritizing SNR in cardiac viability MRIs is only a general guideline, NOT a strict rule. If your patient has trouble holding their breath or has arrhythmias, you may need to prioritize scan time instead. The right balance always depends on the needs of your patient and clinic.
How Contrast Enhancement Works in Cardiac MRI
Cardiac tissue characterization can be done either with or without contrast.
Without contrast, we use mapping sequences like T1, T2, or T2* to assess tissue properties.
With contrast, we give the patient single bolus of gadolinium (Dotarem or Gadovist). Then, we capture images at three specific time points:
Perfusion: Immediately as contrast arrives (0–1 minute)
Early Enhancement: At 2–4 minutes after injection
Late Enhancement: At 10–15 minutes after injection
Each phase reveals different pathology because of how contrast behaves in healthy vs damaged tissue. The following section shows which health conditions each sequence detects.
Health Conditions in Cardiac Tissue Viability – And the MRI Sequences That Reveal Them
The table below lists some of the most common cardiac conditions related to tissue characterization:
Nulls normal myocardium to show chronic damage.
Bright scar tissue defines infarct size and depth.
Key before deciding on revascularization.
Note: For specialized conditions like infiltrative cardiomyopathies (amyloidosis), myocarditis, or iron overload, additional sequences like T1, T2, or T2 mapping would be needed beyond the standard viability protocol for complete tissue characterization.
How to Perform a Cardiac Tissue Characterization Protocol
The step-by-step guide below will show you how to set up and perform contrast-enhanced tissue characterization; the second part of a complete viability assessment.
We will perform the protocol in 3 parts:
Inject the Contrast Agent
Plan and Acquire the Protocol Sequences
Review the Images
Part 1: Inject the Contrast Agent
1. Verify That It’s Safe to Do a Contrast Injection
Before any contrast injection, you must verify that the patient can handle it. Their eGFR must be above 35 mL/min/1.73m², but check your hospital's specific cutoff.
If the patient’s kidneys can't handle the contrast safely, either perform non-contrast tissue characterization or end the exam. Never compromise patient safety for imaging.
2. Prepare and Administer the Contrast Injection
Follow these steps to ensure you prepare and administer the contrast injection correctly:
Prepare All Your Sequences Before Administering the Contrast:
Before injecting the contrast agent, ensure that your sequences are already planned and named correctly. This step ensures that sequences are ready to run immediately after the injection.
Pause the Workflow to Prepare the Contrast Injection:
Use the scanner’s pause function to temporarily stop the imaging workflow. This gives you enough time to prepare and administer the contrast without rushing.
Contrast can be administered either:
Manually: Using a syringe
Automatically: Using an infusion pump, based on your clinic’s setup and protocols.
Prepare the Contrast Agent:
Use Dotarem (0.2 mL/kg, 0.1 mmol/kg) or Gadovist (0.1 mL/kg, 0.1 mmol/kg) as the contrast agent.
Calculate the dosage based on the patient’s weight. For Dotarem, divide the patient’s weight in kg by 5 to get the volume in mL
(e.g., 80 kg ÷ 5 = 16 mL).
Set the contrast agent concentration and injection volume in the scanner’s settings.
Administer the Contrast and Resume Imaging:
After injecting the contrast, place the patient back into the scanner bore, close the door, and return to the console.
Track how much time has passed since injection to ensure you run each sequence at the optimal moment.
Monitor the Patient During Imaging:
While running post-contrast sequences, regularly check the patient for signs of discomfort,
allergic reactions, or irregular breathing patterns.
Part 2: Plan and Acquire the Protocol Sequences
When all preparations are ready, we can start planning and acquiring the protocol sequences.
Let's go through the pulse sequences a standard cardiac tissue viability MRI protocol includes, why we perform them, and how to set them up.
The 9 Sequences of a Standard Cardiac Tissue Viability Protocol
SAX Perfusion GRE (Gradient Echo)
4-chamber Early Enhancement IR-GRE (Inversion Recovery GRE)
2-chamber Early Enhancement IR-GRE
3-chamber Early Enhancement IR-GRE
SAX TI Scout
4-chamber Late Enhancement IR-GRE
2-chamber Late Enhancement IR-GRE
3-chamber Late Enhancement IR-GRE
SAX Late Enhancement IR-GRE
We mainly use Inversion Recovery Gradient Echo (IR-GRE) sequences for this study. This type of sequence makes scarred tissue appear bright, while normal heart muscle appears dark, which makes it easy to spot areas of scarred heart muscle.
These sequences also work with ECG-gating to take pictures between heartbeats, which reduces blurring from heart motion and gives clearer images.
The protocol follows this timeline:
Baseline perfusion images (8–10 phases before contrast)
Inject contrast and continue perfusion (45–50 more phases)
Early enhancement at 2–4 minutes (2ch, 3ch, 4ch)
TI Scout at 8–10 minutes
Late enhancement at 10–15 minutes (2ch, 3ch, 4ch, SAX)
Important! Before injecting the contrast agent, ensure that all your post-contrast sequences are already prepared.
Preparing your sequences beforehand helps you run them at exactly the right time after the injection.
In the sections below, we go through how to plan and set up each sequence.
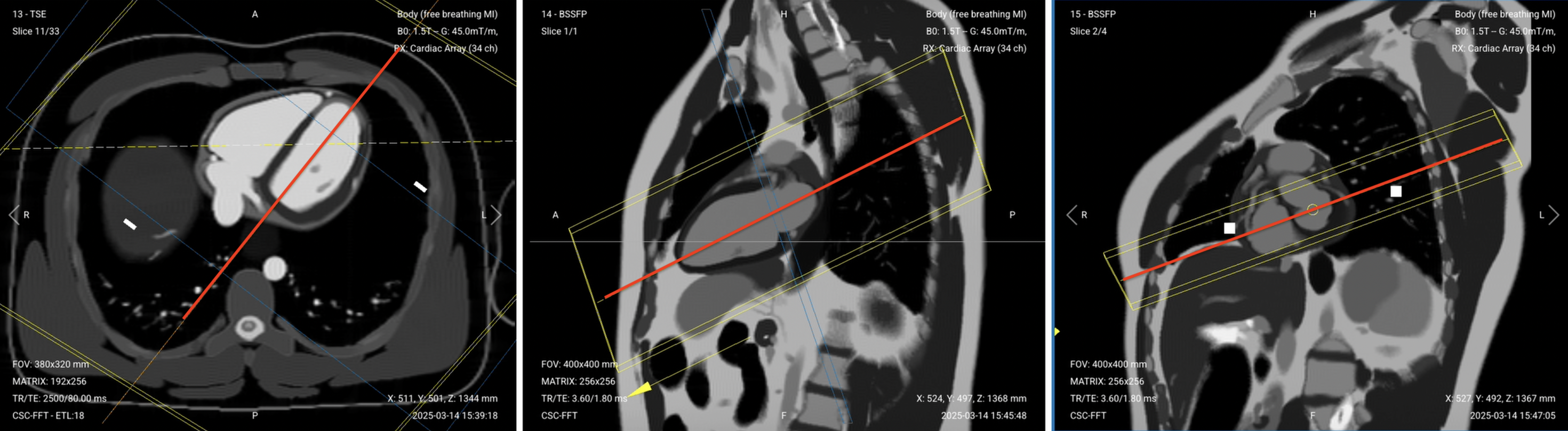
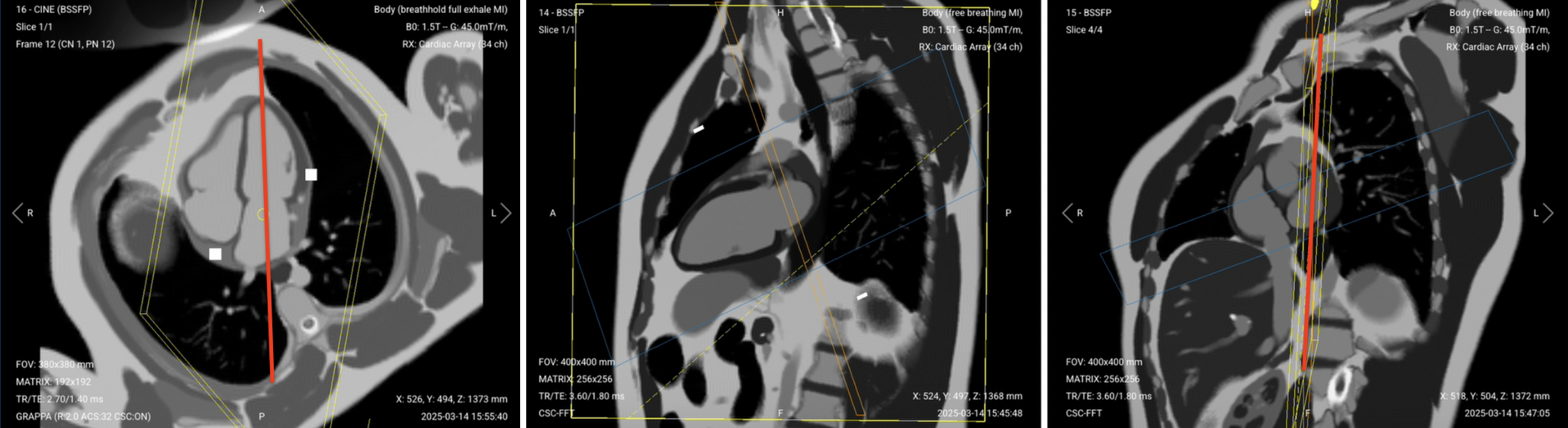
1. Short-Axis (SAX) Perfusion GRE
The perfusion sequence tracks contrast as it flows through the heart muscle. We capture three slices (basal, mid, and apical) to see the entire left ventricle.
Start the perfusion sequence and acquire 8–10 baseline images. Then inject contrast and capture another 45–50 phases as it washes through.
Watch for the contrast arriving in the right ventricle first, then left ventricle, then myocardium. Normal tissue enhances uniformly. Dark areas indicate perfusion defects.
For patients with poor cardiac function, increase phases to 80–100. The slow-moving heart needs more time points to capture the full contrast passage.
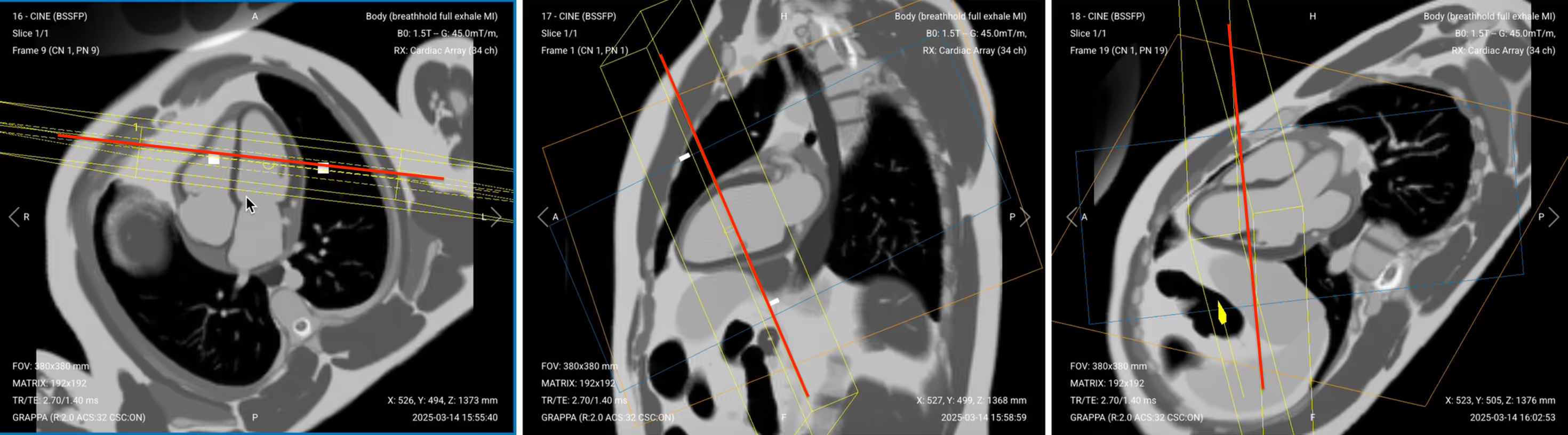
✅ Correct Planning:
Planning Instructions:
Plan the stack using the 2-chamber cine and 4-chamber cine views.
Use the left ventricle and mitral valve as your anatomical references.
Align the slices as follows:
2-chamber cine: Position slices perpendicular to the long axis of the left ventricle. Space them evenly from base to apex.
4-chamber cine: Ensure slices are perpendicular to the interventricular septum and cover the full left ventricle.
Slice thickness: 8–10 mm for adequate coverage with good SNR.
Slice gap: 8–10 mm between slices to avoid overlap while covering the full ventricle.
Set the fold-over direction (phase encoding) to right–left (RL) to minimize wrap artifacts from the chest wall.
Parameters for Short-Axis (SAX) Perfusion:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
2–5 ms
Very short TE to capture rapid contrast passage and minimize T2* effects.
Repetition Time (TR)
5–9 ms
Very short TR enables rapid image acquisition during first-pass perfusion.
Field-of-View (FOV)
360 × 270 mm
Smaller FOV than cine to increase speed while maintaining heart coverage.
Matrix
128 × 96
Low matrix prioritizes temporal resolution over spatial detail for dynamic imaging.
Foldover Direction (Phase)
Right-to-Left (RL)
Reduces wrap artifacts from anterior chest wall during rapid acquisition.
Number of Slices
3
Basal, mid, and apical slices provide full LV coverage efficiently.
Slice Thickness
8–10 mm
Thick slices ensure good SNR during rapid dynamic acquisition.
Slice Gap
8–10 mm
Wide gaps prevent cross-talk while covering the ventricle in 3 slices.
NEX / Averages
1
Single average maximizes temporal resolution for tracking contrast arrival.
Phases
50–60
Captures 50–60 heartbeats. Increase to 80+ for slow hearts or poor function.
Bandwidth
400–700 Hz/pixel
High bandwidth minimizes chemical shift during fast gradient echo acquisition.
Flip Angle
12–15°
Low flip angle maintains steady-state signal during repeated excitations.
Parallel Imaging
GRAPPA 2
Accelerates acquisition for better temporal resolution during first pass.
Saturation Pulse
90° prepulse
Saturates myocardium before each acquisition to enhance contrast arrival.
2. Early Enhancement Sequences (IR-GRE)
Early enhancement shows microvascular obstruction (MVO). These are areas where contrast can't penetrate due to severe acute damage.
Set up three views (2ch, 3ch, 4ch) with very high TI (~440 ms) to make both blood and normal myocardium bright. Any dark spots indicate MVO.
Run these sequences immediately after perfusion finishes, about 2-3 minutes after injection. If you do a manual injection, wait a bit longer (3–4 minutes) since hand-pushing is slower than power injectors.
In healthy patients, both myocardium and blood pool should appear bright. Dark spots within bright myocardium indicate microvascular obstruction, i.e. fresh damage where vessels are blocked.
Planning Instructions:
Copy the slice geometry and planning from the corresponding cine sequences (2ch, 3ch, 4ch).
Keep identical positioning to enable direct comparison with function images.
✅ Correct Planning for 4-Chamber Early Enhancement:
✅ Correct Planning for 2-Chamber Early Enhancement:
✅ Correct Planning for 3-Chamber Early Enhancement:
Parameters for Early Enhancement (All Views):
Parameter
Recommended Values
Why These Values
Echo Time (TE)
3–4 ms
Low TE for gradient echo with good T1 weighting.
Repetition Time (TR)
6–8 ms
Very short TR allows time for inversion recovery while keeping scan time reasonable.
Inversion Time (TI)
400–500 ms
Very high TI brightens blood and healthy tissue so dark MVO spots stand out.
Field-of-View (FOV)
380 × 380 mm
Matches cine FOV for direct comparison of wall motion and enhancement.
Matrix
256 × 192
Higher resolution than perfusion to clearly delineate MVO regions.
Foldover Direction (Phase)
Anterior-to-Posterior (AP)
Consistent with cine acquisitions to maintain comparable geometry.
Number of Slices
1
Single slice per view for 2ch, 3ch, and 4ch orientations.
Slice Thickness
6–8 mm
Matches cine thickness for direct visual comparison.
Slice Gap
1–2 mm
Thin gaps reduce crosstalk and ensure full anatomical coverage between slices.
NEX / Averages
1–2
One average keeps scan time short; a second average may improve SNR if motion is an issue.
Bandwidth
200–400 Hz/px
Moderate bandwidth balances SNR with minimal chemical shift.
Flip Angle
20–25°
Optimized for T1 contrast with inversion preparation.
Trigger Delay
Mid-diastole
Reduces motion artifacts by imaging during the cardiac rest phase.
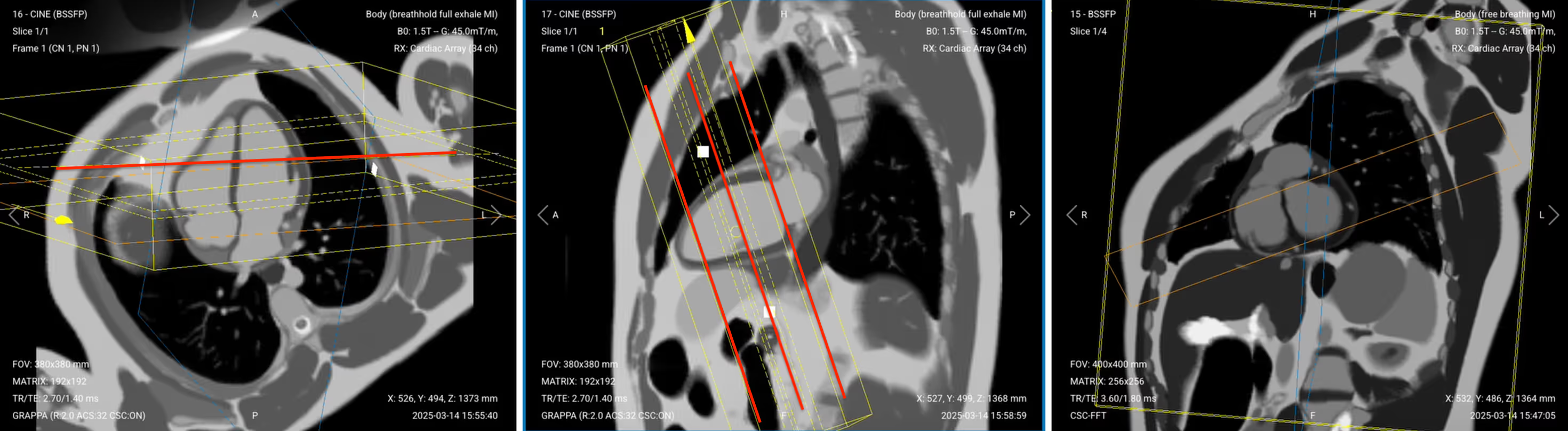
3. TI Scout – Finding the Myocardium Null Point
The TI Scout sequence shows multiple images with different inversion times. The goal is to find the exact timing that nulls healthy myocardium so it appears completely black.
The TI value from this image (typically 200–250 ms at 1.5T) will be used for all late enhancement sequences.
Run the TI Scout 8–10 minutes after contrast injection.
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from your previous SAX cine stack. Start by scrolling through the cine slices and select a mid-ventricular slice to copy; a slice that shows a full ring of myocardium.
Use the left ventricle as your anatomical reference.
In the long-axis view, center on the left ventricle at the papillary muscle level.
Use appropriate geometry parameters:
Slice number: 1 slice at mid-ventricular level.
Slice thickness: 8 mm for good SNR during multiple TI sampling.
Slice gap: Not applicable (single slice).
Set the fold-over direction (phase encoding) to right–left (RL) to match short-axis orientation.
Parameters for TI Scout:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
3–4 ms
Standard for gradient echo with inversion recovery.
Repetition Time (TR)
25–30 ms
Long enough to sample multiple TI values in one acquisition.
TI Range
150–350 ms
Samples every 25 ms to bracket the myocardial null point.
Field-of-View (FOV)
380 × 380 mm
Consistent with other cardiac sequences.
Matrix
128 × 96
Low resolution acceptable since we're finding timing, not anatomy.
Number of Images
8–11
One image per TI value tested across the range.
Slice Thickness
8 mm
Single thick slice for robust signal during TI testing.
Bandwidth
150–300 Hz/pixel
Moderate bandwidth to balance good SNR with reduced chemical shift.
Flip Angle
20°
Balanced for T1 contrast across multiple TI values.
How to Read the TI Scout to Find the Right TI Value
Once your TI Scout has finished running, we must now read the resulting images to find the right TI value.
Scroll through its images and look at the areas where 1) the myocardium interfaces with the blood pool, and 2) the papillary muscles and epicardium cross over.
✅ TI Scout – Correct Image Example:
In these areas, look for these key features:
Myocardium appears darkest
Epicardium can be clearly seen as a bright line (but not too bright)
Chest wall muscles also dark (confirming proper muscle nulling)
Clear distinction between nulled myocardium and bright blood pool
The correct TI for late enhancement typically falls between 200–250 ms at 10–15 minutes post-contrast. Select the value that best nulls the myocardium.
4. Late Enhancement Sequences (IR-GRE)
Late gadolinium enhancement (LGE) is the gold standard for identifying myocardial scar. We acquire the same views as early enhancement but with optimised TI to null healthy muscle.
Use the TI value from your scout to acquire all late enhancement sequences.
Planning Instructions for All Late Enhancement Views:
Copy the slice geometry and planning from the corresponding cine sequences (2ch, 3ch, 4ch, SAX).
Keep identical positioning to enable direct comparison with function images.
Set TI based on the TI Scout result (typically 200–250 ms).
✅ Correct Planning for 4-Chamber Late Enhancement (same as early 4-chamber):
✅ Correct Planning for 2-Chamber Late Enhancement (same as early 2-chamber):
✅ Correct Planning for 3-Chamber Late Enhancement (same as early 3-chamber):
✅ Correct Planning for SAX Late Enhancement:
Parameters for Late Enhancement (All Views):
Parameter
Recommended Values
Why These Values
Echo Time (TE)
3–4 ms
Short TE improves T1 contrast and minimizes flow artifacts.
Repetition Time (TR)
6–8 ms
Very short TR allows time for inversion recovery while maintaining good scan time.
Inversion Time (TI)
200–250 ms
Based on TI Scout. Nulls normal myocardium to highlight scar.
Field-of-View (FOV)
380 × 380 mm
Large enough to cover the heart in long- and short-axis orientations.
Matrix
256 × 192
High enough resolution to clearly outline scar borders.
Foldover Direction (Phase)
AP for 2ch/3ch/4ch, RL for SAX
Prevents aliasing over myocardium; matches foldover to anatomical layout.
Number of Slices
1 per long-axis view; 8–10 for SAX
Single long-axis slices show key walls; SAX stack covers full left ventricle.
Slice Thickness
6–8 mm
Same as cine stack for precise visual comparison.
Slice Gap
1–2 mm for SAX; N/A for long-axis
Thin gap in SAX prevents crosstalk and preserves full coverage.
NEX / Averages
1–2
One average is typical; add second only if motion is present.
Bandwidth
100–250 Hz/px
Medium-low to balance good SNR with reduced chemical shift.
Flip Angle
20–25°
Optimal for T1 weighting with IR prep.
Parallel Imaging
Optional GRAPPA 2
Reduces breath-hold time while maintaining image quality.
Trigger Delay
Mid-diastole
Heart is most still; avoids motion blur in scar regions.
5 Common Mistakes in Cardiac Contrast Enhancement and How to Avoid Them
Mistake 1: Incorrect Inversion Time (TI)
Late gadolinium enhancement only works if the TI is set to fully null the signal from healthy myocardium. Using the wrong value may cause scars to appear faint or blend in with normal tissue.
To get reliable results, always run a TI Scout first and select the recommended time, which is typically 200–250 ms.
Mistake 2: Mismatched Slice Planning
Late enhancement images are meant to be compared directly with cine views from the function study. But if slice plannings don’t match, those comparisons lose value.
You should thus always copy the exact slice positions from your cine sequences for each view, including the 2-chamber, 3-chamber, 4-chamber, and short axis.
Mistake 3: Planning Sequences After Injecting Contrast
Timing is critical once contrast is administered, since each phase must be captured at the right moment.
To keep everything on schedule, all sequences must be fully prepared and positioned before the injection begins.
Mistake 4: Too Few Phases in Perfusion Imaging
Perfusion sequences capture the passage of contrast through the myocardium in real time, so you need enough temporal resolution to follow the entire flow. If the heart is pumping slowly, short sequences may miss part of the wash-in.
To avoid this, increase to at least 60 phases if the patient’s heart is struggling, or the cine images may show sluggish motion.
Mistake 5: Skipping Patient Safety Check Before Contrast
Gadolinium contrast can pose serious risks for patients with impaired kidney function.
Always confirm that the patient’s eGFR is above 35, or your site’s official threshold, before proceeding with any contrast-enhanced sequences. Choose non-contrast options if the patient isn’t cleared.
Part 3: Review the Images
Finally, we will review the images to ensure all the anatomical information we need is clear.
In a cardiac viability tissue characterization MRI, these structures must be clearly visible:
Myocardial scar tissue, including transmural extent and subendocardial involvement
Microvascular obstruction (MVO) zones within infarcted areas
Viable myocardium with normal nulling on late enhancement
Left ventricular walls in all 17 segments per AHA model
Papillary muscles and their enhancement patterns
Pericardium and any pericardial enhancement
Below, we will go through all the different image contrasts and explain their specific role in tissue characterization.
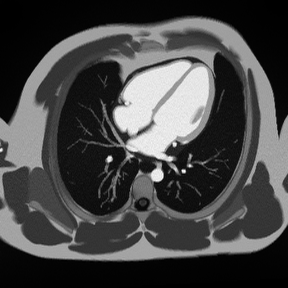
Perfusion Gradient Echo – Shows Real-Time Blood Flow Through Myocardium
Perfusion imaging captures the first pass of contrast agent through the heart muscle. As contrast arrives, normal myocardium enhances quickly and evenly. Areas with poor blood flow remain dark.
In cardiac viability, rest perfusion identifies areas of reduced blood flow caused by scar tissue or ischemia. Dark regions during first-pass indicate either infarcted tissue or severely narrowed arteries.
The contrast between dark viable tissue and bright scar helps determine:
Scar size and location
Transmural extent (how deep the scar goes)
Viability for revascularization; whether myocardium is viable or permanently scarred
We capture perfusion in short-axis views at basal, mid, and apical levels to assess the entire left ventricle.
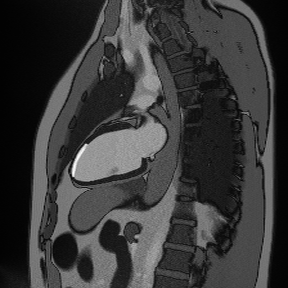
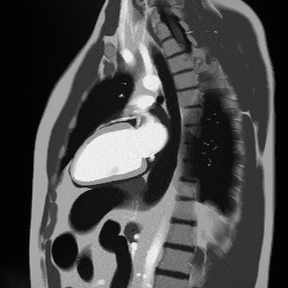
In the frame below, we can see a perfusion defect. This is the black semi-circle border that stretches the top-half of the left ventricle. (The left ventricle is shown on the right side in this image).
To the right, we see that the damage only extends less than 50% through the heart wall, which indicates a sub-endocardial scar. There’s still viable myocardium that may yet recover.
But to the left, the damage stretches across the entire heart wall. This indicates a transmural scar, with no hope hope of recovery.
Things to Look for in Rest Perfusion:
Dark areas that persist throughout contrast arrival indicate perfusion defects
Normal myocardium should enhance uniformly within 1–2 heartbeats
Transmural defects indicate more severe disease or infarction
Early Gadolinium Enhancement – Reveals Acute Injury and Microvascular Obstruction
Early enhancement sequences are acquired 2–4 minutes after contrast injection. At this timing, contrast has entered most tissues but hasn't yet penetrated areas with microvascular obstruction (MVO).
MVO appears as dark zones within bright infarcted tissue. This represents severe microvascular damage where even contrast molecules can't penetrate. Finding MVO is important because it predicts worse outcomes and larger final infarct size.
We acquire early enhancement in 2-chamber, 3-chamber, and 4-chamber views to see MVO from multiple angles.
✅ 4-Chamber Early Gadolinium Enhancement – Correct Image Example:
Things to Look for in 4-Chamber Early Enhancement:
Assess all visible walls for dark MVO zones
Both ventricles should be clearly visible
Look for any pericardial enhancement suggesting inflammation
✅ 2-Chamber Early Gadolinium Enhancement – Correct Image Example:
Things to Look for in 2-Chamber Early Enhancement:
Dark zones within bright areas indicate MVO
Both blood pool and myocardium should appear bright
MVO typically occurs in the core of large infarcts
Size and location help predict recovery potential
✅ 3-Chamber Early Gadolinium Enhancement – Correct Image Example:
Things to Look for in 3-Chamber Early Enhancement:
Check the septum and inferior wall for MVO
Ensure the aortic outflow tract is visible
Compare with late enhancement to track MVO evolution
Late Gadolinium Enhancement (LGE) – The Gold Standard for Scar Detection
Late enhancement imaging takes place 10–15 minutes after contrast injection. By this time, contrast has washed out of normal myocardium but remains trapped in scar tissue.
This sequence helps answer a critical clinical question:
“How much of the heart muscle is permanently damaged?”
To highlight scar tissue clearly, we use the TI Scout to select the correct inversion time (TI) that nulls the signal from healthy myocardium. When done correctly, healthy muscle appears dark, while scar tissue stands out as bright white.
The amount of scar tells us how likely the tissue is to recover after treatment:
Subendocardial scars cover less than 50% of the wall thickness and often regain function after revascularization. Like toast burnt only on one side, they may still be salvageable.
Transmural scars extend more than 50% through the heart wall and rarely recover. Like toast burnt all the way through, this damage is usually permanent and beyond recovery.
To fully understand the location and depth of scarring, we acquire late enhancement images in multiple views.
✅ 4-Chamber LGE – Correct Image Example:
Things to Look for in 4-Chamber LGE:
Evaluate all four chambers for abnormal enhancement
Bright signal in RV insertion points is normal
Check for thrombus (appears dark) adjacent to scar
✅ 2-Chamber LGE – Correct Image Example:
Things to Look for in 2-Chamber Late Enhancement:
Bright areas indicate scar tissue
Measure transmural extent (percentage of wall thickness)
Subendocardial scars appear as bright inner rim
Check inferior and anterior walls
✅ 3-Chamber LGE – Correct Image Example:
Things to Look for in 3-Chamber Late Enhancement:
Assess basal septum and inferolateral wall
Look for scar extension into papillary muscles
Ensure proper nulling of normal myocardium
✅ SAX LGE – Correct Image Example:
Things to Look for in SAX LGE:
Systematically assess all 17 AHA segments
Document scar location, size, and transmural extent
Compare with perfusion defects to identify hibernating myocardium
Look for papillary muscle involvement
Final Checks:
Before finishing a cardiac viability tissue characterization MRI, always check these 5 points to ensure diagnostic quality:
Complete Coverage: All myocardial segments assessed in perfusion, early, and late enhancement from base to apex.
Proper Nulling: Normal myocardium appears uniformly black on late enhancement with TI verified by scout sequence.
Scar Assessment: Transmural extent clearly visible and measurable in all affected segments.
MVO Detection: Early enhancement sequences checked for dark zones within infarcted areas.
Image Quality: All sequences have adequate SNR, sharp borders, and minimal artifacts from arrhythmias or breathing.





.gif)
.avif)
.bmp)