How to plan a brain tumor MRI protocol (part 2: post-contrast)
Written by:
Erik Jacobsson
This step-by-step guide is for MRI students, radiographers, and technologists who wish to improve their planning skills and master the brain tumor MRI protocol.
This guide is Part 2 of planning a brain tumor MRI assessment. In Part 1, we covered pre-contrast imaging and tumor characterization.
In this Part 2, we will follow up with contrast injection and post-contrast imaging, where we identify enhancement patterns that guide tumor diagnosis and treatment planning.
What you will learn:
Key factors in brain tumor MRIs, including trade-offs.
How to perform the contrast injection workflow
Best post-contrast pulse sequences and planning techniques.
Ways to avoid common artifacts.
Qualities of great brain tumor images.
Key Takeaways
Resolution and SNR are nearly equal priorities, with resolution slightly ahead.
Missing a 2 mm brain metastasis can completely change treatment decisions.
High spatial detail is essential to differentiate tumor types and detect infiltrative margins.
SNR is not a goal on its own, but it must be high enough to support the required resolution.
Scan time ranks third, unless patient motion becomes a problem.
Most patients tolerate around 30 minutes of scanning.
However, motion can make images completely unreadable.
For uncooperative patients, it is better to sacrifice some resolution or SNR than lose the entire study to motion blur.
Brain tumor protocols rely on many complementary sequences.
No single sequence gives a complete picture.
We apply 3D T1 for anatomy and contrast comparison, T2 for edema and cystic components,
FLAIR for infiltrative margins, diffusion-weighted imaging for cellularity,
and T2 star for hemorrhage.
Together, these contrasts reveal different tissue properties of the tumor.
Avoid these common brain tumor MRI artifacts.
Artifacts
Solution – How to Avoid It
Motion artifacts
Shorten the scan time to reduce the risk of patient movement.
Immobilize the patient as much as possible with foam pads.
Susceptibility artifacts
Use spin echo sequences rather than gradient echo when possible.
Position DWI slices to avoid air-tissue interfaces at skull base.
Chemical shift artifacts
Increase the bandwidth to reduce the spatial displacement between fat and water signals.
CSF flow artifacts
Use flow compensation gradients and fast sequences like FLAIR to minimize CSF pulsation effects.
Truncation artifacts
Increase the resolution to capture more frequency information and reduce Gibbs ringing at tissue boundaries.
Wrap-around artifacts
Activate fold-over suppression to prevent anatomy outside the field of view from overlapping.
Geometric distortion (on diffusion-weighted imaging)
Use parallel imaging to reduce echo train length and susceptibility buildup.
Use a short TE to reduce distortion from inhomogeneous magnetic fields.
Intro to Post-Contrast Brain Tumor Imaging
In Part 1 of our brain tumor protocol, we completed all pre-contrast sequences. We captured baseline anatomical information with 3D MP-RAGE, assessed tumor composition with T2 and FLAIR, evaluated cellularity with diffusion-weighted imaging, and checked for hemorrhage with T2* gradient echo.
Now we continue with another core part of brain tumor assessment: contrast-enhanced imaging. This is where we identify enhancement patterns that guide diagnosis and treatment planning.
Enhancement patterns help us distinguish between different tumor types:
Rim enhancement: High-grade glioma, abscess, or metastasis
Homogeneous enhancement: Meningioma or lymphoma
No enhancement: Low-grade glioma
These patterns directly impact treatment decisions and prognosis.
How to Balance the 3 Trade-offs in Brain Tumor MRIs
In MRI, we always face a trade-off between 3 key metrics:
Scan Time: How fast a pulse sequence can be completed.
Resolution: How much detail the image can display.
SNR: How clear the image is, how much signal relative to noise.
Improving one of these metrics reduces the performance of the others. To decide what trade-offs to make, we must consider the needs of each clinical situation.
For brain tumor MRIs, we face these challenges:
Missing a 2 mm metastasis could change treatment entirely. We need to see small lesions clearly and detect infiltrative margins that extend into normal brain tissue.
We must differentiate between different tumor types based on their signal characteristics. This requires adequate image clarity to distinguish subtle differences in tissue properties.
Brain tumor protocols are comprehensive studies that include many sequences. Most patients can tolerate around 30 minutes of scanning, but beyond that, motion artifacts can make images completely unreadable.
Therefore, we typically:
Prioritize resolution to detect small metastases and infiltrative margins,
Keep good SNR to ensure adequate image clarity for our resolution targets, and
Optimize scan time as needed to stay within the practical limit of around 30 minutes.
Note! Prioritizing resolution in brain tumor MRIs is only a general guideline, NOT a strict rule. If the patient cannot hold still, then scan time becomes the top priority. For uncooperative patients, it's better to sacrifice some resolution or SNR than to risk motion blur that makes images completely unreadable. The right balance always depends on the needs of your patient and clinic.
Post-Contrast Brain Tumor Conditions and the MRI Sequences That Reveal Them
These are some of the most common brain tumor conditions we look for in post-contrast imaging, and which pulse sequences reveal them:
Fat suppression removes bright skull base fat and marrow signal.
This makes thin dural enhancement and the dural tail much easier to see.
The Contrast Injection Workflow
Understanding the complete workflow helps you plan efficiently and avoid delays after contrast injection. The key principle is: plan all post-contrast sequences before injecting contrast.
For Manual Injection:
Insert cannula in patient's arm
Position patient at isocenter
Acquire all pre-contrast sequences
Plan all post-contrast sequences
Slide patient table out of bore
Enter scan room with prepared syringe
Inject contrast slowly through cannula
Press isocenter button to reposition patient
Return to control room and start post-contrast acquisitions (about 3-5 min after starting the injection)
For Automated Power Injection:
Insert cannula in patient's arm
Connect IV line from injector to cannula
Position patient at isocenter
Acquire all pre-contrast sequences
Plan all post-contrast sequences
Set injection parameters (volume, flow rate, etc.)
Initiate injection from control room
Wait 3-5 minutes after starting injection, then start post-contrast sequences
In both workflows, Step 4 (planning post-contrast sequences) happens before contrast injection. This ensures zero wasted time after injection.
How to Perform Brain Tumor Contrast-Enhanced Imaging
The step-by-step guide below will show you how to perform contrast-enhanced imaging for brain tumor assessment, the second part of a complete brain tumor protocol.
In Part 1, we set up the patient, captured localizer images, and acquired all pre-contrast sequences. Now in Part 2, we will perform the protocol in 3 parts:
Plan and Set Up the Post-Contrast Sequences
Inject the Contrast Agent
Review the Images
Part 1: Plan and Set Up the Post-Contrast Sequences
Before we inject contrast, we must plan all post-contrast sequences and have them ready to run. This ensures we don’t waste any time after injection.
The 3 post-contrast sequences of a standard brain tumor MRIs:
Sagittal T1 3D MP-RAGE
Axial T1 TSE with Fat Suppression
Coronal T1 TSE with Fat Suppression
We use T1-weighted sequences after contrast because they show enhancement patterns that guide diagnosis.
3D MP-RAGE is the gold standard for tumor enhancement and abnormal blood-brain barrier breakdown. The fat-suppressed T1 TSE sequences confirm enhancement patterns and eliminate fat signal that could obscure pathology.
In the sections below, we go through how to plan and set up each sequence.
1. Planning Sagittal T1 3D MP-RAGE (Post-Contrast)
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from the pre-contrast sagittal T1 3D MP-RAGE sequence.
Keep the same slice angulation, coverage, and positioning to ensure precise comparison between pre- and post-contrast images.
Use identical spatial resolution and planning to enable side-by-side overlay comparison.
Parameters for Post-Contrast Sagittal T1 3D MP-RAGE:
Use the same parameters as the pre-contrast T1 3D MP-RAGE sequence to ensure the post-contrast sequences maintain the same appearance and can be clearly compared.
Parameter
Recommended Values
Why These Values
Echo Time (TE)
3–4 ms
Very short TE minimizes T2* effects and maximizes T1 contrast.
Repetition Time (TR)
1,800–2,500 ms
Long TR allows complete relaxation between inversion pulses in MP-RAGE sequence.
Inversion Time (TI)
800–900 ms
Optimizes gray-white matter contrast at 3T by nulling gray matter at the right time.
Field-of-View (FOV)
230 × 230 mm
Square FOV for isotropic voxels, large enough to cover the entire brain.
Matrix
232 × 232
High matrix combined with small voxels provides excellent spatial resolution for isotropic imaging.
Foldover Direction (Phase)
Anterior-to-Posterior (AP)
Minimizes FOV in AP direction to reduce scan time while covering brain fully.
Number of Slices
124–192
Enough slices to cover the brain with 1–1.2 mm thickness for isotropic resolution.
Slice Thickness
1–1.2 mm
Thin slices for isotropic voxels enable multiplanar reconstruction in any plane. Ideally aim for 1 mm cubic voxels.
Slice Gap
0 mm
Contiguous slices for 3D acquisition ensure no gaps in coverage.
NEX / Averages
1
Single average keeps scan time reasonable while maintaining good SNR at 3T.
Flip Angle
15°
Low flip angle optimizes T1 contrast with short TR in gradient echo sequence.
Bandwidth
200–250 Hz/px
Medium bandwidth balances chemical shift and SNR.
Parallel Imaging
Optional GRAPPA/SENSE factor 2
Can reduce scan time by approximately 50% while maintaining image quality if needed.
Fold-over Suppression
Yes
Prevents wrap-around artifacts from posterior structures.
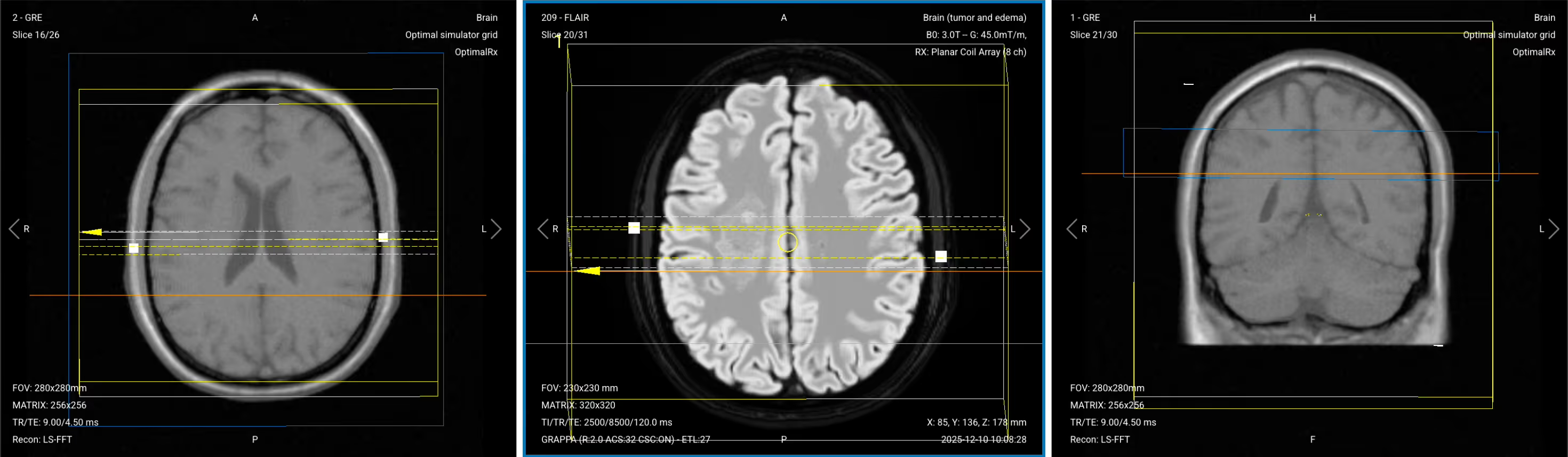
2. Planning Axial T1 TSE with Fat Suppression (Post-Contrast)
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from the axial T2 TSE sequence.
Keep the same slice angulation, coverage, and positioning to ensure images can be easily compared with other axial sequences.
This sequence should be acquired at approximately 10-12 minutes post-injection for peak parenchymal enhancement.
Parameters for Post-Contrast Axial T1 TSE with Fat Suppression:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
8–12 ms
Short TE is required for T1 contrast.
Repetition Time (TR)
350–600 ms
Short TR is required for T1 contrast.
Field-of-View (FOV)
210 × 250 mm
Large enough to cover the brain while avoiding wrap-around artifacts.
Matrix
320 × 320
High matrix provides excellent spatial resolution for detecting small lesions.
Foldover Direction (Phase)
Right-to-Left (RL)
Reduces wrap-around artifacts and optimizes FOV for brain shape.
Number of Slices
30–35
Enough slices to fully cover from vertex to foramen magnum.
Slice Thickness
3–4 mm
Thinner than routine brain (typically 5–6 mm) for better tumor detail.
Slice Gap
0–1 mm
Minimal gap provides continuity between slices while avoiding cross-talk.
NEX / Averages
3
Higher averaging improves SNR for detecting subtle enhancement.
Turbo Factor / ETL
3–5
Low turbo factor maintains T1 weighting and avoids T2 contamination.
Bandwidth
244 Hz/px
Medium bandwidth balances SNR with chemical shift artifacts.
Refocusing Flip Angle
180°
Standard refocusing angle for TSE sequences.
Fold-over Suppression
Yes
Prevents wrap-around artifacts from posterior structures.
Fat Suppression
Spectral
Eliminates fat signal to make true contrast enhancement clearly visible.
3. Planning Coronal T1 TSE with Fat Suppression (Post-Contrast)
✅ Correct Planning:
Planning Instructions:
Use the post-contrast sagittal T1 3D MP-RAGE for planning.
Align the slices as follows:
Sagittal Localizer: Perpendicular to the midsagittal line of the brain.
Axial Localizer: Ensure slices run from anterior (frontal lobe) to posterior (occipital lobe) without cutting out any anatomy.
Use appropriate geometry parameters:
Slice number: Enough to cover from the posterior fossa to the frontal lobe (typically 20-25 slices).
Slice thickness: 6 mm, medium thickness for good resolution without sacrificing scan time or SNR.
Slice gap: 1 mm, approximately 20% of slice thickness to provide continuity and avoid cross-talk.
Set the fold-over direction (phase encoding) to right-left (RL) to minimize wraparound artifacts and allow the smallest field of view.
This sequence should be acquired at approximately 13-15 minutes post-injection.
Parameters for Post-Contrast Coronal T1 TSE with Fat Suppression:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
8–12 ms
Short TE is required for T1 contrast.
Repetition Time (TR)
350–600 ms
Short TR is required for T1 contrast.
Field-of-View (FOV)
230 × 220 mm
Optimized for coronal orientation covering brain from anterior to posterior.
Matrix
320 × 224
High matrix provides excellent spatial resolution for detecting small enhancing lesions.
Foldover Direction (Phase)
Right-to-Left (RL)
Minimizes wraparound artifacts and optimizes FOV for brain shape in coronal view.
Number of Slices
30–35
Enough slices to fully cover from posterior fossa to frontal lobe.
Slice Thickness
4 mm
Medium thickness balances resolution with SNR and scan time.
Slice Gap
1 mm
Minimal gap provides continuity between slices while avoiding cross-talk.
NEX / Averages
3
Higher averaging improves SNR for detecting subtle enhancement.
Turbo Factor / ETL
3–5
Low turbo factor maintains T1 weighting and avoids T2 contamination.
Bandwidth
244 Hz/px
Medium bandwidth balances SNR with chemical shift artifacts.
Refocusing Flip Angle
180°
Standard refocusing angle for TSE sequences.
Fold-over Suppression
Yes
Prevents wrap-around artifacts from posterior structures.
Fat Suppression
Spectral
Eliminates fat signal to make true contrast enhancement clearly visible. If spectral fat suppression fails at 3 Tesla, use STIR or inversion recovery instead.
How to Avoid Artifacts When Planning the Sequences
The table below lists the 7 common brain tumor artifacts, and what techniques you can use to avoid them:
Artifacts
Solution – How to Avoid It
Motion artifacts
Shorten scan time to reduce patient movement.
Immobilize the head as much as possible to maintain image sharpness.
Susceptibility artifacts
Use spin echo sequences over gradient echo.
Position slices carefully to reduce effects from air–tissue interfaces.
Chemical shift artifacts
Increase the bandwidth to reduce spatial misregistration between fat and water signals.
CSF flow artifacts
Apply flow compensation gradients and fast sequences such as FLAIR
to reduce cerebrospinal fluid pulsation effects.
Truncation artifacts
Increase spatial resolution to capture more frequency information
and reduce Gibbs ringing at sharp tissue boundaries.
Wrap-around artifacts
Activate fold-over suppression to prevent anatomy outside the field of view
from overlapping the brain.
Geometric distortion (on diffusion-weighted imaging)
Use parallel imaging to reduce echo train length and susceptibility buildup.
Use a short TE to reduce distortion from inhomogeneous magnetic fields.
Part 2: Inject the Contrast Agent
Now that all post-contrast sequences are planned and ready, we proceed with contrast injection following the workflow outlined earlier.
1. Verify Patient Safety
Before any contrast injection, you must verify that the patient can handle it. Their eGFR must be above 35 mL/min/1.73m², but check your hospital's specific cutoff.
If the patient's kidneys can't handle the contrast safely, either perform non-contrast tissue characterization or end the exam. Never compromise patient safety for imaging.
2. Contrast Dosing
Use standard gadolinium at 0.5 millimole per milliliter concentration.
The standard dose is 0.1 millimole per kilogram of patient weight, which typically means 15-20 mL for an 80 kg patient.
3. Timing Protocol
After contrast injection, follow this timing:
Wait 3-5 minutes from the start of injection before starting the 3D MP-RAGE
The 3D MP-RAGE takes ~5-6 minutes to acquire
Start axial T1 with fat suppression at ~10-12 minutes post-injection (immediately after 3D completes)
Acquire coronal T1 with fat suppression at ~13-15 minutes post-injection
This timing provides peak parenchymal enhancement and helps distinguish between different tumor types.
Part 3: Review the Post-Contrast Images
Note! This section only reviews the post-contrast images. See our Part 1 article for the pre-contrast review.
Finally, we will review the images to ensure all the anatomical information we need is clear.
These key structures must be clearly visible in a brain tumor MRI:
Tumor location, margins, and extent
Mass effect and structural distortion
Ventricular compression or shift
Relationship to eloquent cortex and major vessels
Internal tumor composition (solid versus cystic)
Edema and infiltrative margins
Enhancement patterns
Below, we will go through all the different image contrasts and explain their specific role in imaging brain tumors.
Post-Contrast T1 3D MP-RAGE – Reveals Enhancement Patterns
Post-contrast T1 imaging is the gold standard for detecting tumor enhancement and abnormal blood-brain barrier breakdown.
In brain tumor imaging, post-contrast T1 3D MP-RAGE reveals enhancement patterns that guide diagnosis and tumor grading. Rim enhancement with a central hypointense core suggests high-grade glioma, abscess, or metastasis. Homogeneous enhancement indicates meningioma, lymphoma, or some metastases.
Absence of enhancement suggests low-grade glioma, though some high-grade gliomas also show minimal enhancement. Nodular enhancement appears in hemangioblastomas and some cystic lesions. The thin 1 mm slices allow detection of subtle enhancement and enable multiplanar reconstructions for detailed assessment.
We acquire this sequence in sagittal orientation because it provides volumetric coverage that can be reconstructed in any plane while maintaining isotropic resolution.
✅ Sagittal T1 3D MP-RAGE (Post-Contrast) – Correct Image Example:
Things to Look for in Post-Contrast T1 3D MP-RAGE:
Enhancement pattern (rim, homogeneous, nodular, or absent)
Dural tail sign suggesting meningioma
Vascular encasement or invasion
Small enhancing foci suggesting microadenomas or metastases
Compare carefully with pre-contrast T1 to distinguish true enhancement from intrinsic T1 hyperintensity
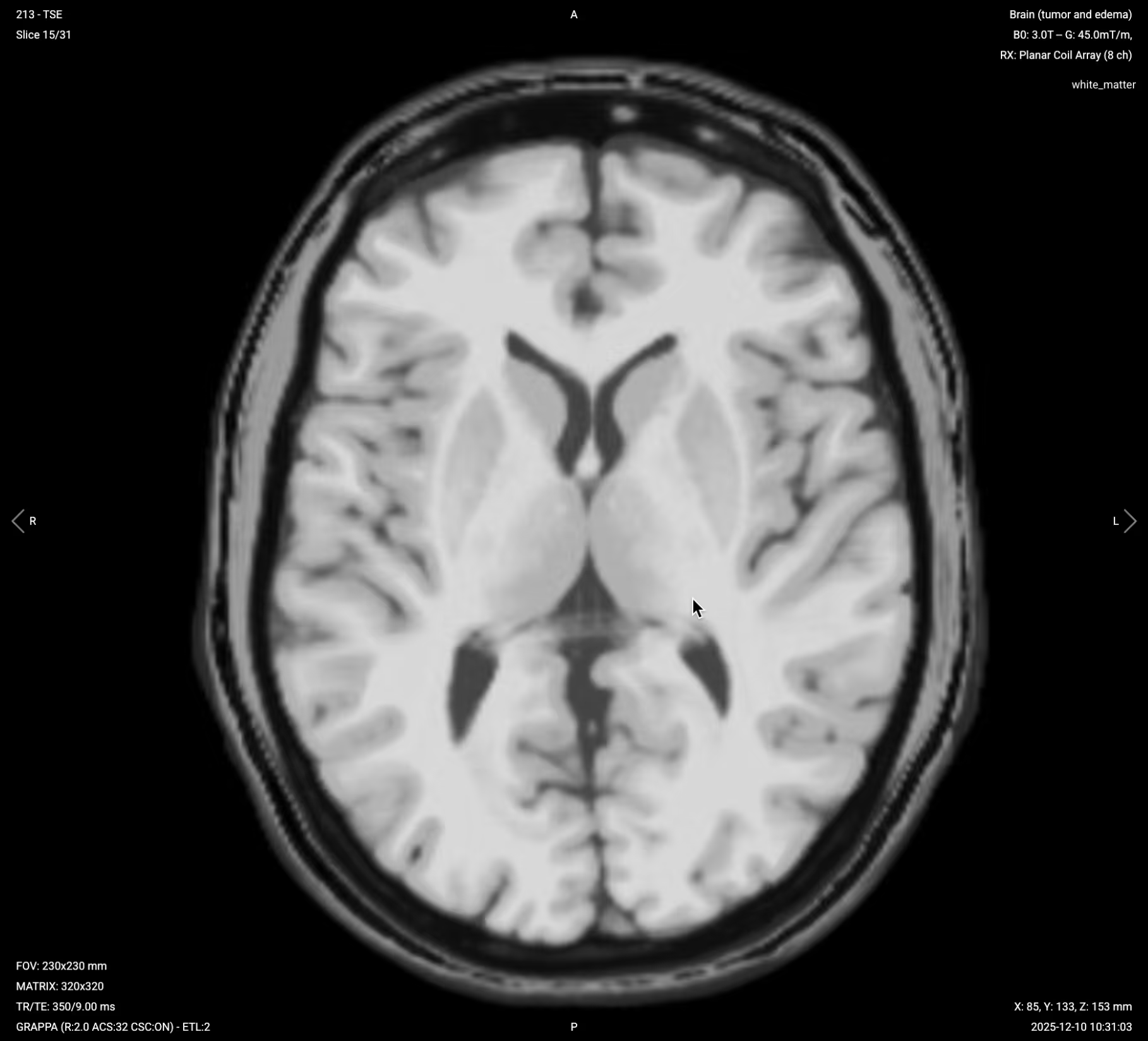
Post-Contrast Axial T1 with Fat Suppression – Confirms Enhancement Patterns
Post-contrast T1 with fat suppression eliminates bright signal from fat, making true contrast enhancement stand out more clearly.
In brain tumor imaging, axial post-contrast T1 with fat suppression confirms enhancement patterns seen on the 3D MP-RAGE from a different angle. Fat suppression helps distinguish true enhancement from fat or hemorrhage, particularly near the skull base or in extraaxial tumors. This sequence provides peak parenchymal enhancement when acquired at 10-12 minutes post-injection, making subtle tumor enhancement more visible.
We acquire this sequence in axial orientation to match other standard axial sequences and enable direct comparison with pre-contrast images.
Things to Look for in Post-Contrast Axial T1 with Fat Suppression:
Confirmation of enhancement patterns from different angle
Subtle enhancement that may be obscured by fat without suppression
Clear distinction between enhancement and hemorrhage or fat
Relationship of enhancing tumor to surrounding structures
Absence of fat signal near skull base clarifying true enhancement
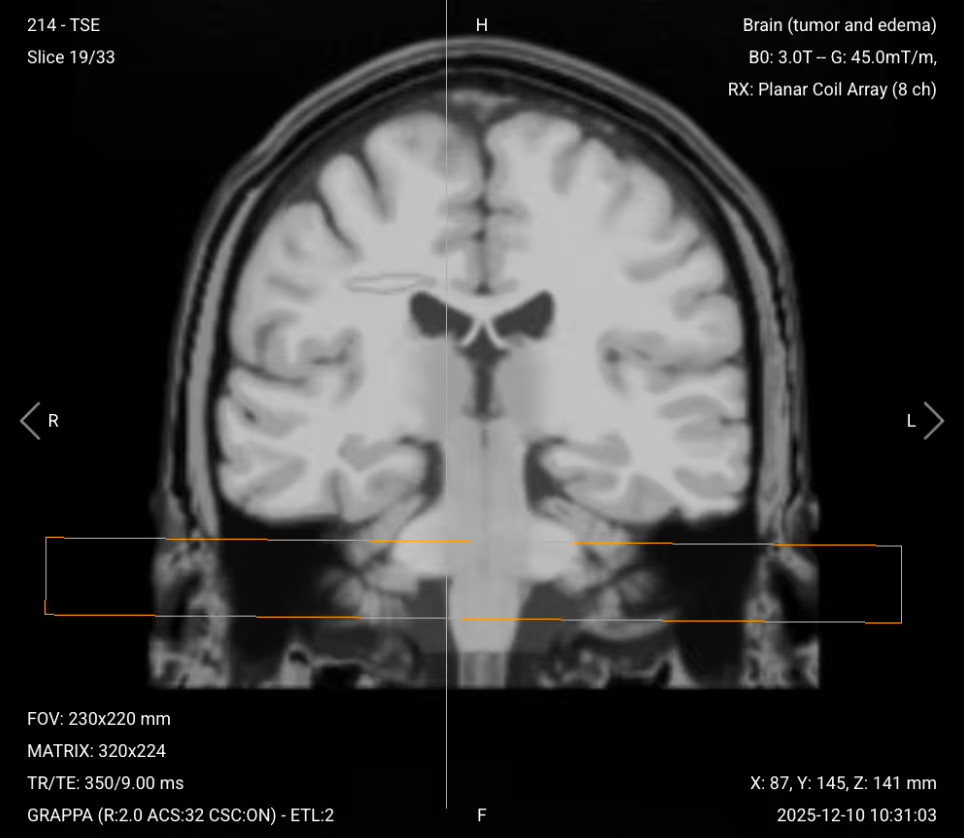
Post-Contrast Coronal T1 with Fat Suppression – Assesses Superior-Inferior Extent
Post-contrast coronal T1 with fat suppression provides a frontal perspective of tumor enhancement with fat signal eliminated.
In brain tumor imaging, coronal post-contrast T1 with fat suppression assesses the superior-inferior extent of the tumor and its enhancement. This view is particularly useful for identifying dural involvement, meningeal spread, and skull base invasion. Fat suppression clarifies enhancement along the meninges and skull base where fat might otherwise obscure pathology. This sequence complements the sagittal and axial post-contrast images for complete three-dimensional assessment.
We acquire this sequence in coronal orientation to complete the three orthogonal planes and provide optimal assessment of superior-inferior tumor relationships.
Things to Look for in Post-Contrast Coronal T1 with Fat Suppression:
Superior-inferior tumor extent and enhancement
Dural involvement or meningeal spread along brain surface
Skull base invasion
Relationship to cranial nerves and vascular structures
Final Checks
Before finishing a post-contrast brain tumor MRI, always check these 6 points to ensure diagnostic quality:
Pre- and Post-Contrast Comparison: Pre-contrast and post-contrast T1 images must have identical planning to enable accurate comparison and enhancement assessment.
Complete Coverage: All sequences must fully cover the entire tumor and surrounding brain tissue, with no anatomical structures cut off.
Enhancement Pattern Clarity: Post-contrast images must clearly show enhancement patterns, with adequate timing (peak parenchymal enhancement at 10-12 minutes post-injection).
Multiplanar Assessment: Tumor must be evaluated in all three planes (axial, sagittal, coronal) for complete spatial understanding.
Fat Suppression Quality: Post-contrast sequences with fat suppression must show uniform fat suppression, making true enhancement clearly visible.
Image Quality and Artifacts: Images must have strong SNR, crisp detail, and minimal motion, chemical shift, susceptibility, or wrap-around artifacts. Motion artifacts are particularly critical to control in brain tumor protocols.





.avif)