This step-by-step guide is for MRI students, radiographers, and technologists who wish to improve their planning skills and master the cervical spine MRI protocol.
What you will learn:
Key factors in cervical spine MRIs, including trade-offs.
Patient and scanner setup tips.
Best pulse sequences and planning techniques.
Ways to avoid common artifacts.
What great cervical spine images should look like.
Key Takeaways
Slightly prioritize resolution to see fine anatomical structures.
C-spine imaging needs sharp images to catch tiny disc protrusions or early cord compression. SNR comes next for tissue contrast, and scan time is last in priority.
We mainly use Turbo/Fast Spin Echo sequences in cervical spine MRIs.
These give fast, high-quality images with strong soft tissue contrast. They support T1, T2, and STIR contrast, helping us detect issues like compression, herniation, and inflammation.
Avoid these 5 common cervical spine artifacts.
Artifacts
Solution – How to Avoid It
CSF flow artifacts
Set the fold-over direction foot-to-head to align with CSF flow direction.
Motion artifacts
Place saturation bands on the throat to reduce swallowing artifacts.
Wrap-around artifacts
Activate fold-over suppression to prevent anatomy outside the field of view from overlapping.
Chemical shift artifacts
Increase the bandwidth (220 Hz at 1.5T, 440 Hz at 3T).
Truncation artifacts
Increase the matrix size to capture more frequency information.
Intro to Cervical Spine MRIs
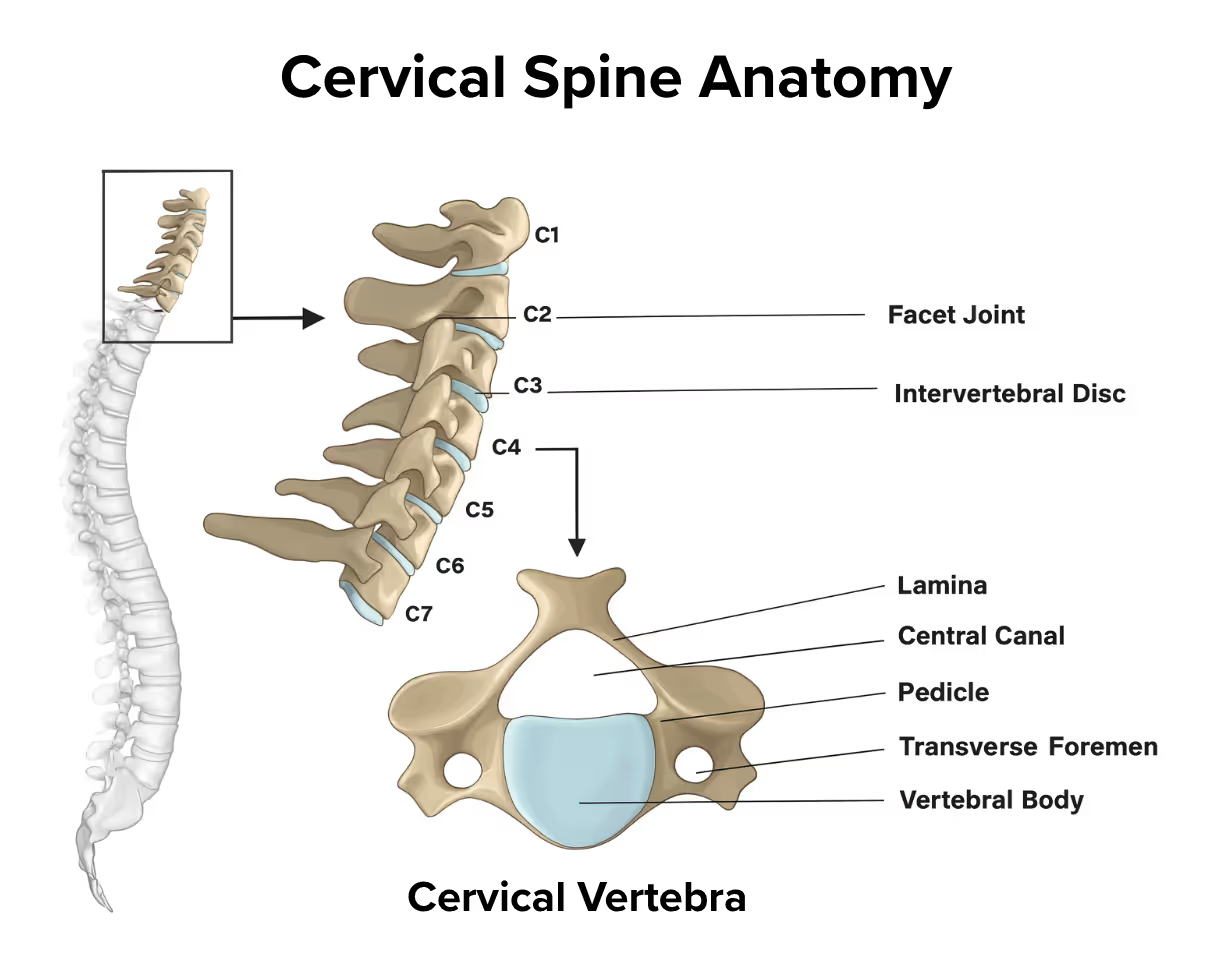
The cervical spine consists of seven vertebrae (C1-C7) that support the head and protect the spinal cord in the neck region. This area is highly mobile and vulnerable to injury from trauma, degenerative changes, and various pathological processes.
Because of its critical role in supporting the head and protecting vital neural structures, the cervical spine is one of the most frequently examined areas in MRI. Imaging helps assess disc herniation, spinal stenosis, cord compression, traumatic injuries, and other conditions that can significantly impact neurological function and quality of life.
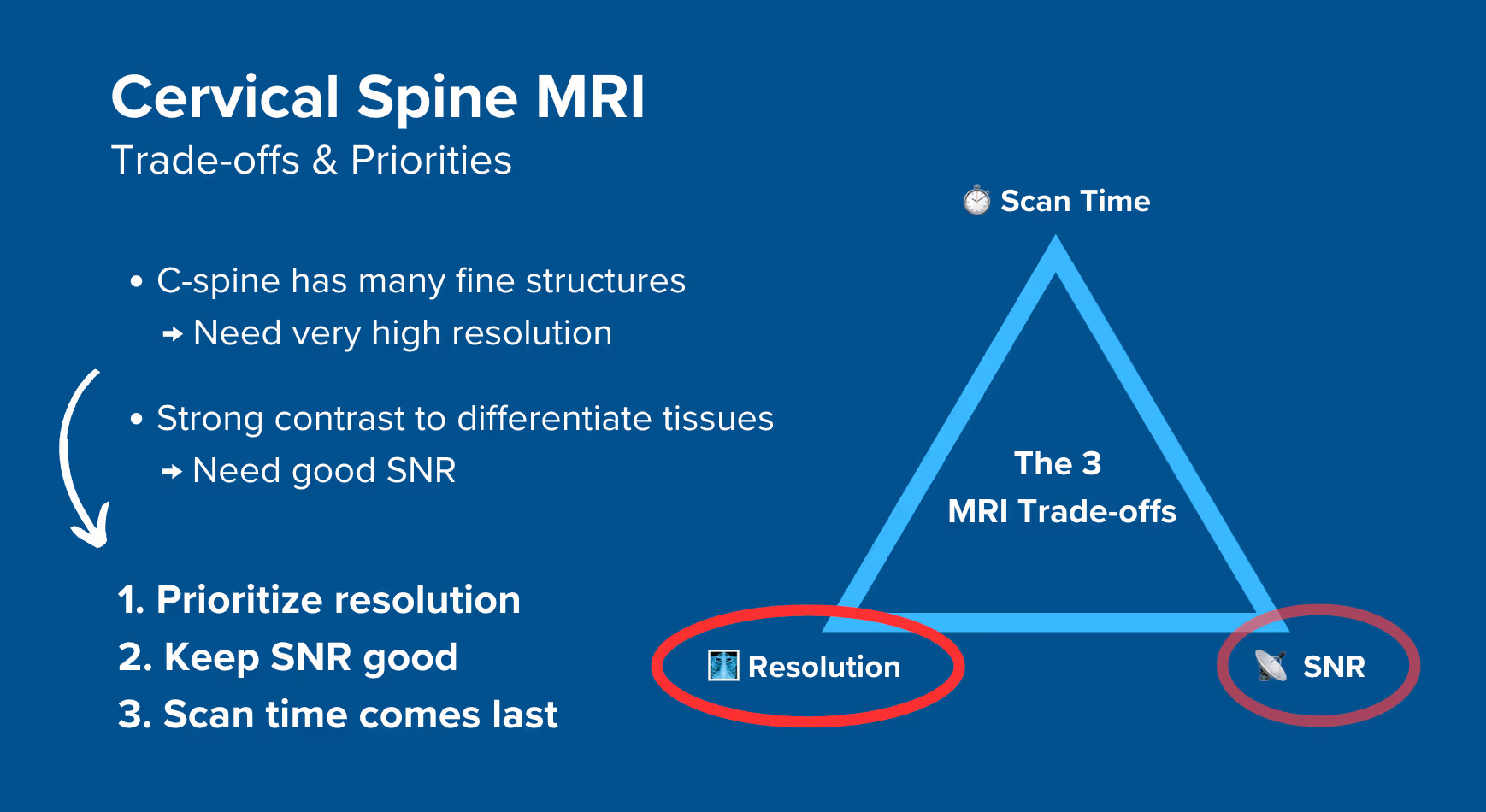
How to Balance the 3 Trade-offs in Cervical Spine MRIs
In MRI, we always face a trade-off between 3 key metrics:
Scan Time: How fast a pulse sequence can be completed.
Resolution: How much detail the image can display.
SNR: How clear the image is, how much signal relative to noise.
Improving one of these metrics reduces the performance of the others. To decide what trade-offs to make, we must consider the needs of each clinical situation.
For cervical spine MRIs: We need to visualize fine anatomical structures like disc herniations, nerve root compression, and subtle spinal cord changes. Some of these structures are only a few millimeters wide. Without good resolution, we might miss conditions like small disc protrusions or early cord compression.
Signal-to-noise ratio is also important because we need strong tissue contrast to differentiate between the spinal cord, cerebrospinal fluid, disc material, and nerve roots. Poor SNR makes it harder to see pathology against normal structures.
Therefore, we typically:
Slightly prioritize resolution to see fine details and nerve compressions,
Maintain good SNR to ensure clear tissue contrast between structures, and
Optimize scan time last while keeping it reasonable since patient motion can blur our images.
Note! Prioritizing resolution in cervical spine MRIs is only a general guideline, NOT a strict rule. At 3T, we gain significant signal that can be invested to improve resolution further or reduce scan time. The right balance always depends on your magnetic field strength, patient cooperation, and clinical needs.
Cervical Spine Health Conditions and the MRI Sequences That Reveal Them
Makes CSF appear bright, clearly showing compression as narrowing of bright fluid around the spinal cord. Excellent contrast between cord, CSF, and disc material reveals stenosis and herniations.
Acute trauma and inflammatory conditions:
• Ligament tears
• Cord contusions
• Acute vertebral fractures
• Bone marrow edema
STIR TSE
Nulls fat signal completely while highlighting water-rich inflamed tissue. Makes edema and acute trauma changes highly visible against suppressed fat background. More robust than spectral fat suppression.
Structural and anatomical changes:
• Chronic fractures
• Bone marrow pathology
• Subacute hemorrhage
T1 TSE (Pre-contrast)
Highlights fat and provides clear anatomical detail. Shows bone marrow composition and structural integrity. Provides baseline anatomy before contrast administration.
Enhancing lesions and vascular abnormalities:
• Spinal tumors
• Metastases
• Active infections
• Vascular malformations
T1 TSE (Post-contrast)
Shows active blood supply through enhancement. Tumors and metastases enhance due to increased vascularity. Active infections enhance while chronic scarring does not, differentiating active from inactive disease.
1.5T vs 3T – What Changes at Higher Field Strengths?
This guide provides parameter recommendations for both 1.5T and 3T systems throughout the protocol sections. All example images shown are acquired at 3T to show the enhanced image quality achievable with higher field strength.
When we move from 1.5T to 3T, three important things change:
1. Signal Gain Doubles and Priorities Change
At 3T, we gain roughly double the signal compared to 1.5T. This extra signal changes our trade-off priorities.
Since we now have more signal than we need, SNR drops to third priority. We can invest the extra signal to either increase resolution (see finer details) or reduce scan time while maintaining the same quality.
For cervical spine imaging, we typically invest this signal gain into improved resolution to better visualize fine anatomical structures like small disc herniations and nerve root compression.
2. Frequency Precession Differences Double
The frequency precession difference between fat and water spins doubles from ~220 Hz at 1.5T to ~440 Hz at 3T.
This means we must increase our bandwidth/px to around 440 Hz to prevent chemical shift artifacts.
3. T1 Relaxation Times Are Prolonged
At higher magnetic field strengths, most tissues (including fat) have longer T1 relaxation times. This means it takes longer for magnetization to recover after an inversion pulse.
This specifically affects STIR sequences, which use an inversion recovery pulse to null fat signal. The TI must be timed to catch fat magnetization at the exact moment it crosses zero (null point).
Since fat takes longer to relax at 3T, we need a longer TI (around 180–220 ms) to hit that null point. If we used the 1.5T TI value at 3T, we'd null the fat too early and get incomplete fat suppression.
Key Parameter Adjustments for 3T
Parameter
1.5T Value
3T Value
Why the Change
Bandwidth/px
~244 Hz
~434 Hz
Must match the doubled frequency precession difference to prevent chemical shift artifacts.
STIR Inversion Time (TI)
130–180 ms
180–220 ms
T1 relaxation times are prolonged at 3T, requiring longer TI for optimal fat nulling.
Field of View
240 × 240 mm (square)
160 × 200 mm (rectangular)
Smaller FOV at 3T improves resolution while maintaining coverage. Rectangular shape matches spine anatomy.
Matrix
320 × 272
288 × 272
Can use smaller matrix at 3T while achieving better resolution due to reduced FOV.
Averages / NEX
1–2
1
Single average sufficient at 3T due to signal gain, reducing scan time.
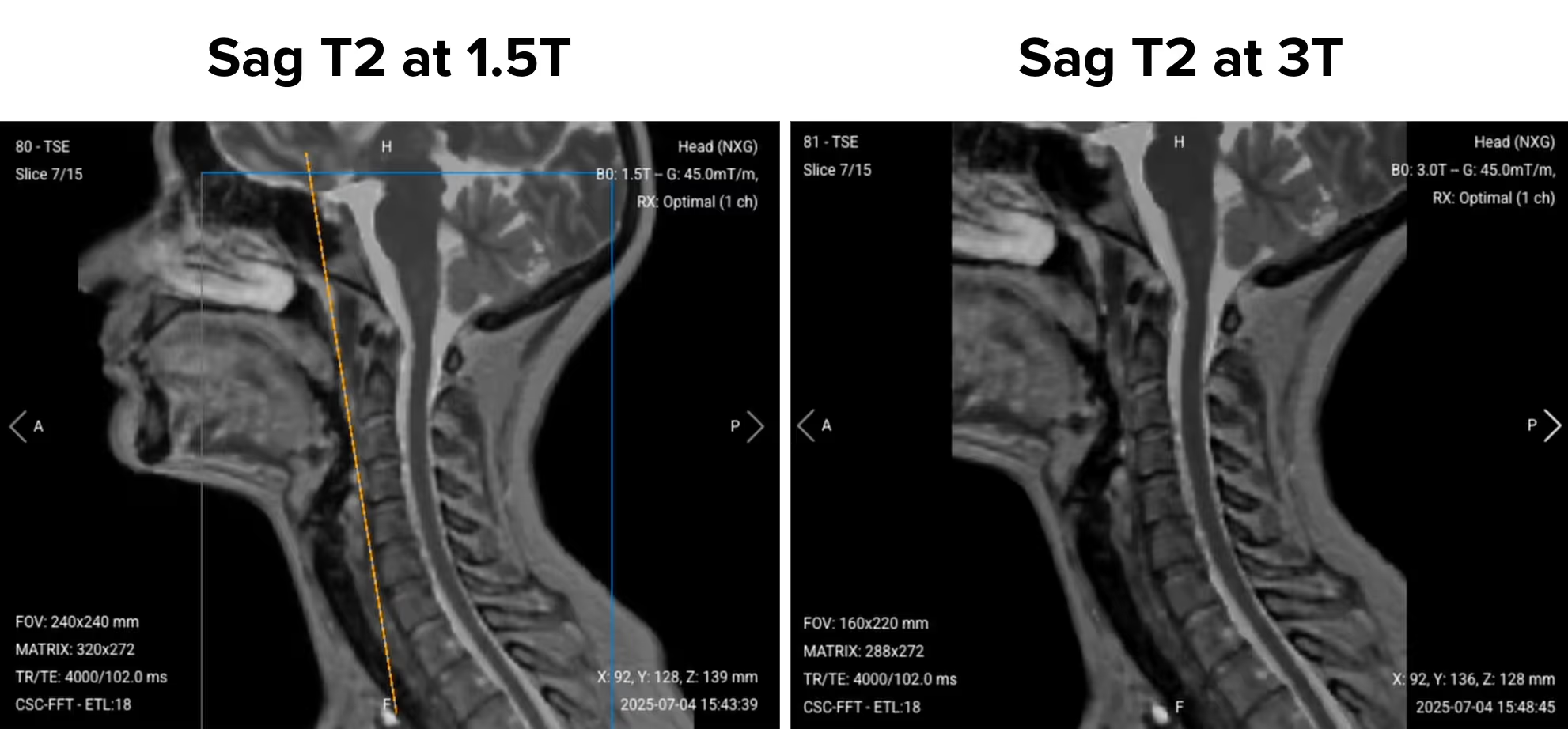
1.5T vs 3T – Image Quality Comparison
The images below show sagittal T2 TSE sequences acquired at both field strengths, demonstrating the resolution and scan time improvements achievable at 3T:
What parameters were used to acquire the above images:
Faster scanning: 50% reduction in scan time improves patient comfort and workflow
Maintained image quality: Despite lower relative SNR, image quality remains diagnostic due to improved resolution
3T allows us to prioritize resolution while simultaneously reducing scan time, giving us the best of both improvements.
How to Perform a Cervical Spine MRI
The step-by-step guide below will show you how to set up and perform a cervical spine MRI protocol in practice.
We will perform the protocol in 3 parts:
Set up the Patient and MRI Scanner
Plan and Acquire the Protocol Sequences
Review the Images
Part 1: Set up the Patient and MRI Scanner
1. Position the Patient in the Scanner
Lay the patient head-first and supine (on their back) with the head and neck centered at the scanner's isocenter.
The positioning for cervical spine examinations is similar to how we position a patient for neuro examinations, as we use the same coil system.
Use a dedicated brain coil with extension to ensure high-resolution imaging. The brain coil offers an extension that goes from the vertex of the head down to the cervical spine segment, providing strong signal reception and full coverage of the cervical region.
Once the patient is in place, review your scanner’s hardware settings.
In this guide, we will use the following settings:
Scanner Setting
Value
Why This Value
Magnetic field strength
1.5 or 3 T
1.5 T enables high Signal-to-Noise Ratio, which gives superior image quality.
3T provides roughly double the signal for improved resolution or reduced scan time.
Maximum gradient strength
45 mT/m
Enables faster acquisitions while preserving high image quality.
This hardware setup is widely used in clinical practice. It balances acquisition time, image quality, and patient comfort.
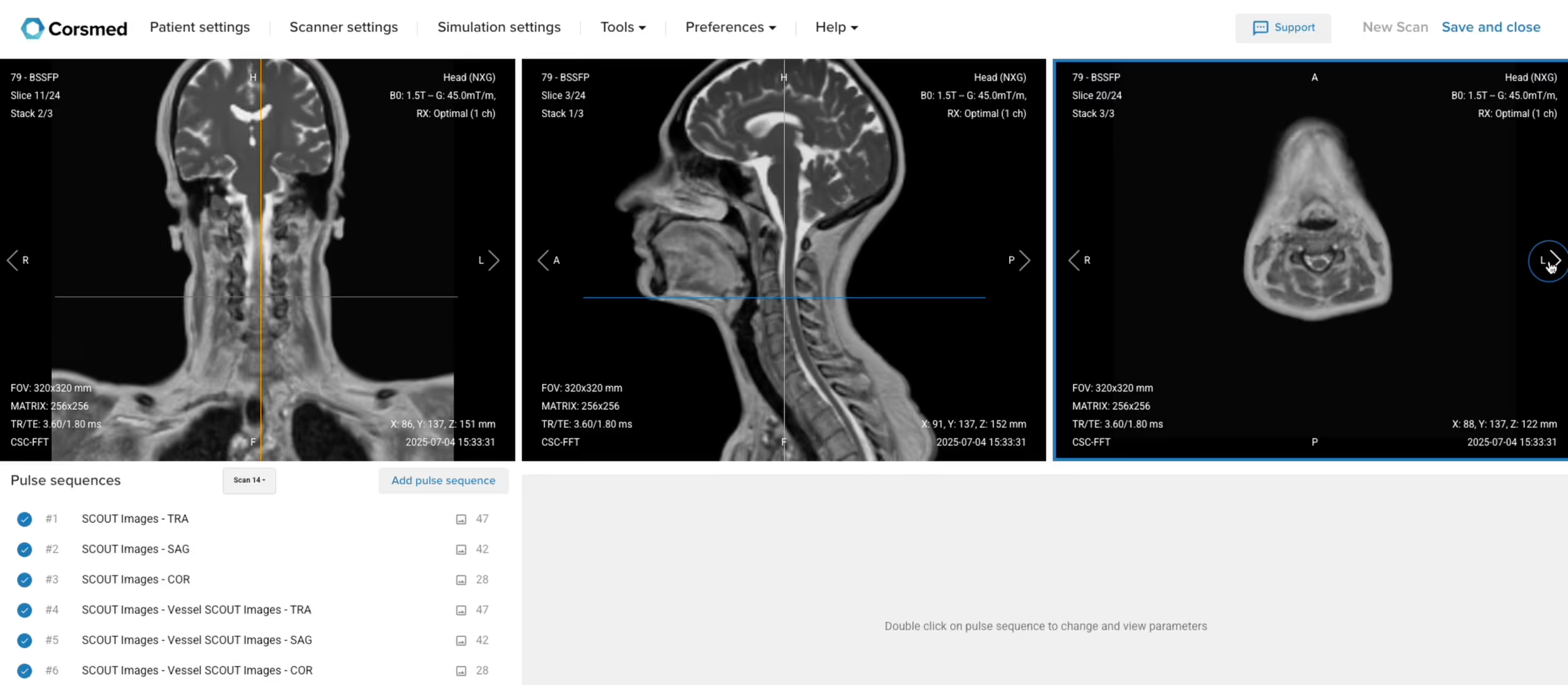
3. Capture the Initial Localizer Images
Before we can perform any MRI protocol, we must always capture initial localizer images of the patient. These images act as a guide for planning the detailed scans we will perform next.
We should always capture localizers in three planes:
Axial
Sagittal
Coronal
Once acquired, upload the initial localizer images into the three viewports.
Then, scroll through each of the image stacks to locate a central slice that clearly shows the anatomy of the cervical spine.
✅ Correct Setup of Localizer Images for Cervical Spine MRI:
Part 2: Plan and Acquire the Protocol Sequences
When all preparations are ready, we can start planning and acquiring the protocol sequences.
Let's go through the pulse sequences a standard cervical spine MRI protocol includes, why we perform them, and how to set them up.
The 6 Sequences of a Standard Cervical Spine MRI Protocol
Sagittal T2 TSE
Sagittal T1 TSE
Sagittal STIR TSE
Coronal T2 TSE
Axial T2 TSE
Axial T1 TSE
We mainly use Turbo/Fast Spin Echo sequences for this study. These sequences provide fast, high-quality images with excellent soft tissue contrast and minimal artifacts, making them ideal for cervical spine diagnosis.
Turbo Spin Echo also lets us create multiple types of contrasts, including T2, T1, and inversion recovery for fat suppression. This helps us assess the spine's structure, detect abnormalities, and identify common pathologies like disc herniation, cord compression, and inflammation.
In the sections below, we go through how to plan and set up each sequence.
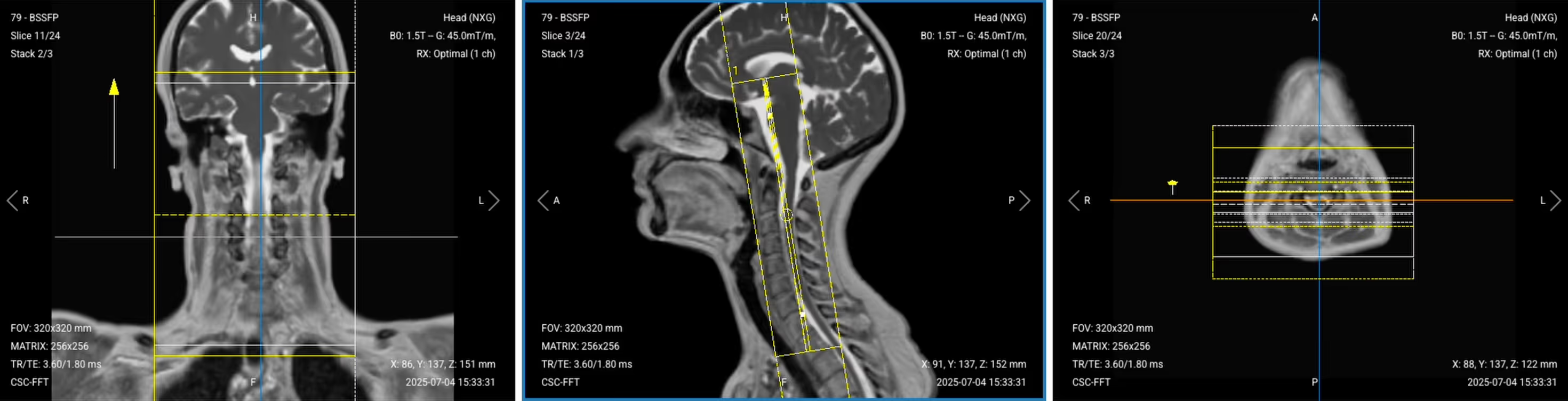
1. Planning Sagittal T2 TSE
✅ Correct Planning:
Planning Instructions:
Use the spinal cord as your anatomical reference.
Align the slices as follows:
Coronal localizer: Grab the slice and align it parallel to the spinal cord direction.
Axial localizer: Ensure the line passes through the middle of the vertebral body, following all the way back to the posterior processes of the vertebrae.
Use appropriate geometry parameters:
Slice number: Enough to cover vertebral bodies from right to left (typically 15–20 slices).
Slice thickness: 3 mm, optimal for good resolution without sacrificing scan time or SNR.
Slice gap: 0.3 mm, minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
Set the fold-over direction (phase encoding) to foot-to-head (FH) to align with CSF flow direction and minimize flow artifacts.
Parameter
Recommended Values
Why These Values
Echo Time (TE)
80–120 ms
Long TE is required for T2 contrast.
Repetition Time (TR)
3,000–5,000 ms
Long TR is required for T2 contrast.
Field-of-View (FOV)
240 × 240 mm (1.5T)
160 × 200 mm (3T)
At 1.5T: Square FOV covers from pons to T1–T2.
At 3T: Rectangular FOV reflects spine structure with improved resolution.
Matrix
320 × 256 (1.5T) 320 × 224 (3T)
High matrix provides good in-plane resolution for detailed anatomical assessment.
Foldover Direction (Phase)
Foot-to-Head (FH)
Aligns with CSF flow direction to minimize flow artifacts.
Slice Thickness
3 mm
Medium thickness for good resolution without sacrificing scan time or SNR.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
NEX / Averages
1–2 (1.5T) 1 (3T)
At 1.5T: 1–2 averages for good image quality.
At 3T: Single average sufficient due to signal gain.
Bandwidth
244 Hz/px (1.5T)
434 Hz/px (3T)
Matches frequency precession difference:
~220 Hz at 1.5T, ~440 Hz at 3T.
Turbo Factor / ETL
15–25
High turbo factor maintains reasonable scan time while preserving T2 contrast.
Fold-over Suppression
Yes
Prevents wrap-around artifacts from anatomy outside the field of view.
2. Planning Sagittal T1 TSE
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from the previous sagittal T2 sequence.
Keep the same slice angulation, coverage, and positioning to ensure images of different contrasts can be clearly compared.
Parameter
Recommended Values
Why These Values
Echo Time (TE)
10 ms
Short TE is required for T1 contrast, highlighting fat-containing tissues.
Repetition Time (TR)
500–800 ms (3T)
At 3T, T1 relaxation gets prolonged, requiring longer TR than at 1.5T.
Field-of-View (FOV)
240 × 240 mm (1.5T)
160 × 200 mm (3T)
At 1.5T: Square FOV covers from pons to T1–T2.
At 3T: Rectangular FOV reflects spine structure with improved resolution.
At 1.5T: Square FOV covers from pons to T1–T2.
At 3T: Rectangular FOV reflects spine structure with improved resolution.
Matrix
320 × 256 (1.5T) 320 × 224 (3T)
High matrix provides good in-plane resolution for detailed anatomical assessment.
Foldover Direction (Phase)
Foot-to-Head (FH)
Aligns with CSF flow direction to minimize flow artifacts.
Slice Thickness
3 mm
Medium thickness for good resolution without sacrificing scan time or SNR.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
NEX / Averages
1–2 (1.5T)
1 (3T)
At 1.5T: 1-2 averages for good image quality.
At 3T: Single average sufficient due to signal gain.
Bandwidth
244 Hz/px (1.5T)
434 Hz/px (3T)
Matches frequency precession difference:
~220 Hz at 1.5T, ~440 Hz at 3T.
Turbo Factor / ETL
2
Lower turbo factor works with shorter echo time of 10 ms.
Fold-over Suppression
Yes
Prevents wrap-around artifacts.
3. Planning Sagittal STIR TSE
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from the previous sagittal T1 sequence.
Keep the same slice angulation, coverage, and positioning to ensure images of different contrasts can be clearly compared.
Parameter
Recommended Values
Why These Values
Echo Time (TE)
80–120 ms
Long TE required for STIR contrast after inversion recovery.
Repetition Time (TR)
3,000–5,000 ms
Long TR required for STIR contrast with inversion recovery.
Inversion Time (TI)
130–180 ms (1.5T) 180–220 ms (3T)
At 1.5T: 130–180 ms.
At 3T: increases to 180–220 ms.
Set to ~200 ms at 3T for optimal fat nulling.
Field-of-View (FOV)
240 × 240 mm (1.5T) 160 × 200 mm (3T)
At 1.5T: Square FOV covers from pons to T1–T2.
At 3T: Rectangular FOV reflects spine structure with improved resolution.
Matrix
256 × 192 (1.5T) 256 × 160 (3T)
Slightly reduced matrix while maintaining good spatial resolution for STIR imaging.
Foldover Direction (Phase)
Foot-to-Head (FH)
Aligns with CSF flow direction to minimize flow artifacts.
Slice Thickness
3 mm
Medium thickness for good resolution without sacrificing scan time or SNR.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
NEX / Averages
1–2
May need additional average due to signal loss from fat suppression.
Bandwidth
150–200 Hz/px (1.5T)
300–400 Hz/px (3T)
Slightly lower than theoretical value to recover SNR lost from fat suppression.
Turbo Factor / ETL
15–25
Optimized for selected echo time and inversion recovery.
Fold-over Suppression
Yes
Prevents wrap-around artifacts.
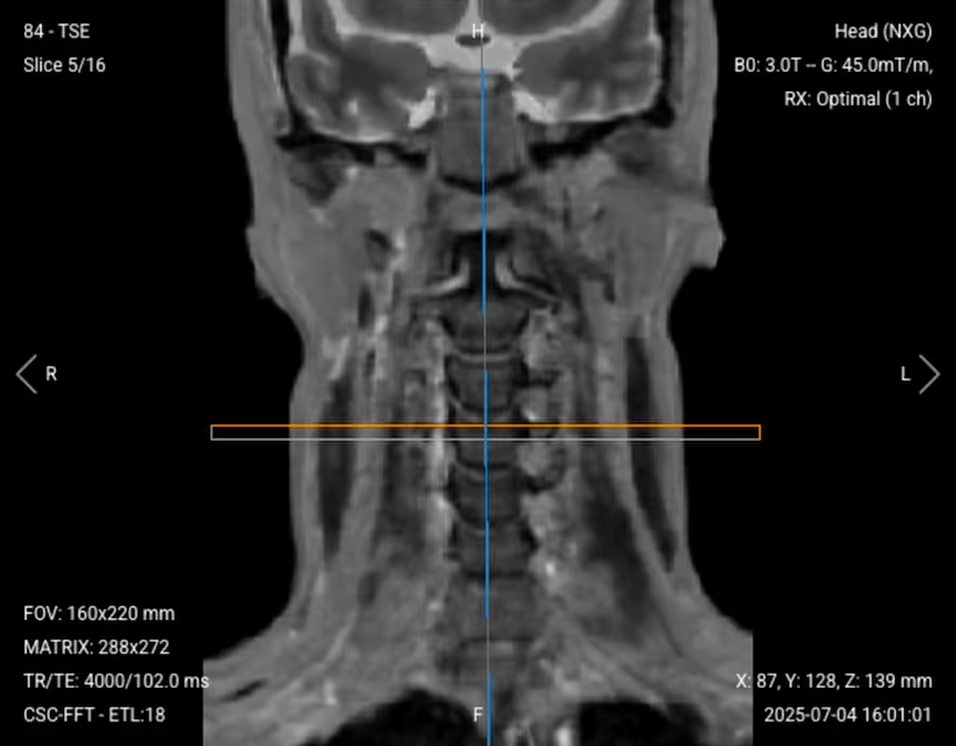
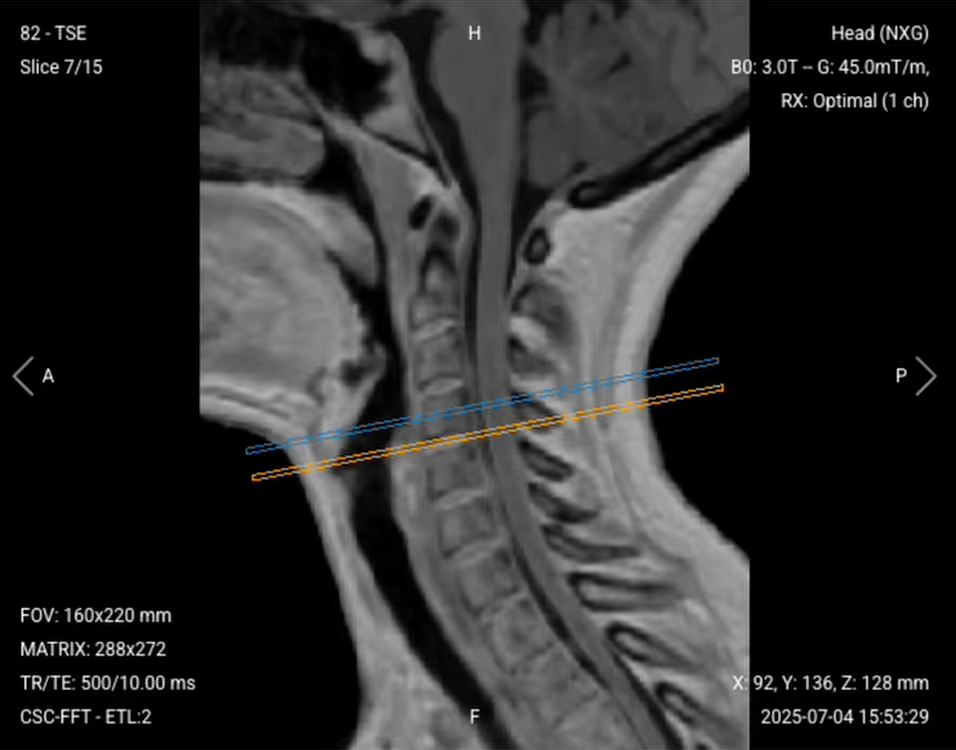
4. Planning Coronal T2 TSE
✅ Correct Planning:
Planning Instructions:
Use the spinal cord as your anatomical reference.
Align the slices as follows:
Sagittal localizer: Align slices parallel to the spine and center them.
Axial localizer: Slices should be perpendicular to the midline that passes through the vertebral body to the posterior processes.
Use appropriate geometry parameters:
Slice number: Enough to cover from anterior cervical spine to posterior (typically 15–25 slices).
Slice thickness: 3 mm, consistent with sagittal sequences.
Slice gap: 0.3 mm, maintains consistency with other sequences.
Set the fold-over direction (phase encoding) to foot-to-head (FH) to avoid flow artifacts, same as sagittal sequences.
Parameter
Recommended Values
Why These Values
Echo Time (TE)
80–120 ms
Long TE required for T2 contrast.
Repetition Time (TR)
3,000–5,000 ms
Long TR required for T2 contrast.
Field-of-View (FOV)
180 × 220 mm
Rectangular shape focused on cervical region, matches spine anatomy.
Matrix
320 × 256 (1.5T) 288 × 272 (3T)
High matrix provides good in-plane resolution for detailed anatomical assessment.
Foldover Direction (Phase)
Foot-to-Head (FH)
Aligns with CSF flow direction to minimize flow artifacts.
Slice Thickness
3 mm
Medium thickness for good resolution without sacrificing scan time or SNR.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
NEX / Averages
1–2 (1.5T)
1 (3T)
At 1.5T: 1-2 averages for good image quality.
At 3T: Single average sufficient due to signal gain.
Bandwidth
244 Hz/px (1.5T)
434 Hz/px (3T)
Matches frequency precession difference: ~220 Hz at 1.5T, ~440 Hz at 3T.
Turbo Factor / ETL
15–25
Higher turbo factor aligns with effective echo time.
Fold-over Suppression
Yes
Prevents wrap-around artifacts.
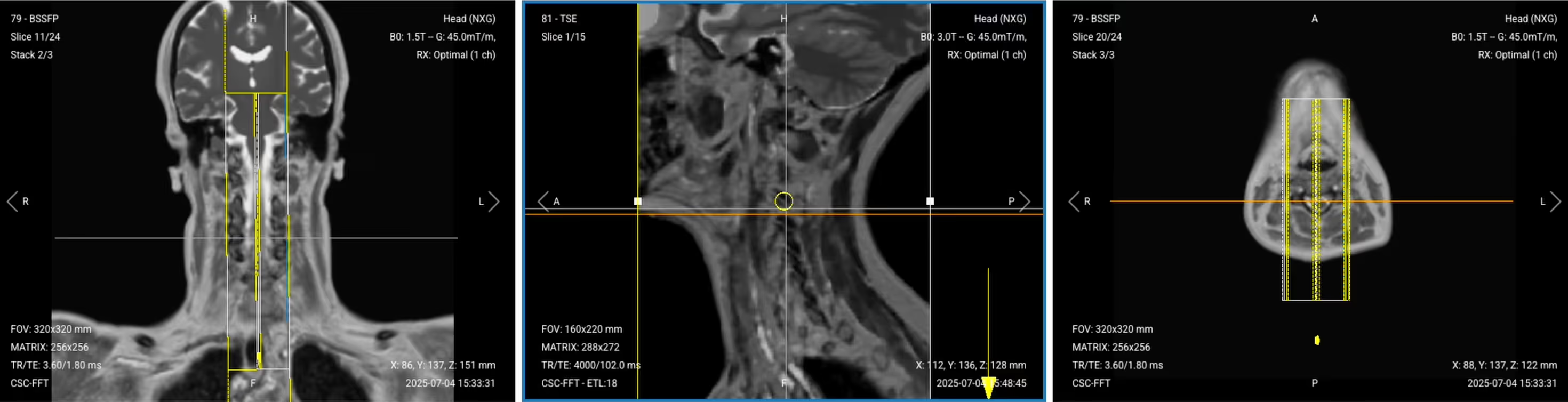
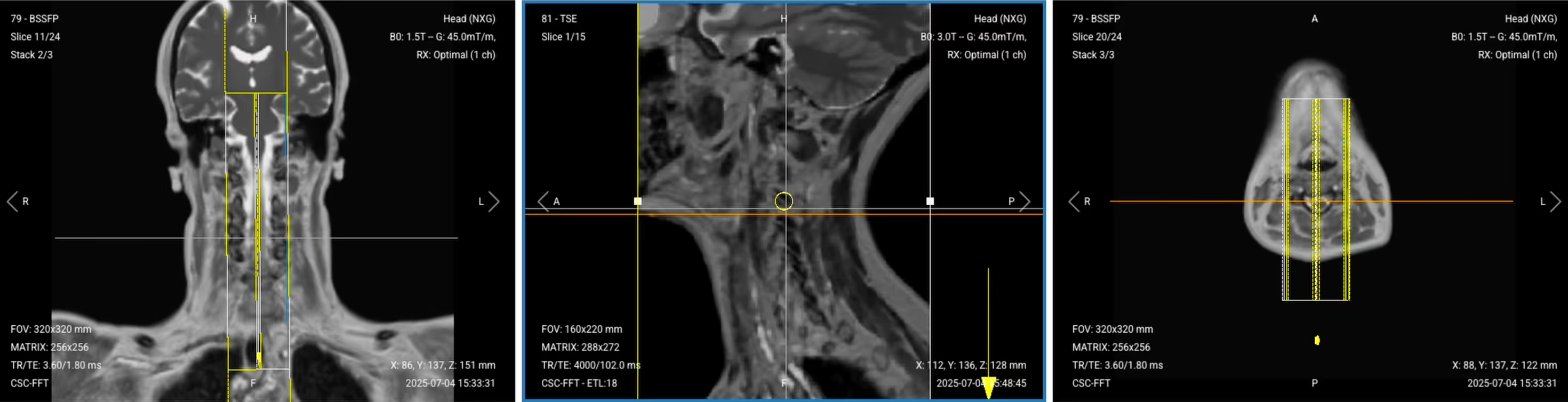
5. Planning Axial T2 TSE
✅ Correct Planning:
Planning Instructions:
Use the cervical spine and intervertebral discs as your anatomical references.
Align the slices as follows:
Sagittal localizer: Slices should be perpendicular to the cervical spine.
Coronal localizer: Slices should run parallel to the intervertebral spaces.
Use appropriate geometry parameters:
Slice number: Enough to cover all seven cervical discs (C1-C7), typically 20–25 slices.
Slice thickness: 3 mm, same as other sequences.
Slice gap: 0.3 mm, maintains consistency.
Set the fold-over direction (phase encoding) to anterior-posterior (AP) to align with the axial anatomy shape.
Place a saturation band on the patient's throat to suppress swallowing artifacts without covering the cervical discs.
Parameter
Recommended Values
Why These Values
Echo Time (TE)
80–120 ms
Long TE required for T2 contrast.
Repetition Time (TR)
3,000–5,000 ms
Long TR required for T2 contrast.
Field-of-View (FOV)
160 × 140 mm
Reduced FOV aligns with axial anatomy shape.
240 × 240 mm (1.5T) 160 × 200 mm (3T)
At 1.5T: Square FOV covers from pons to T1–T2.
At 3T: Rectangular FOV reflects spine structure with improved resolution.
Matrix
320 × 256 (1.5T) 260 × 224 (3T)
High matrix maintains consistent resolution for detailed axial assessment.
Foldover Direction (Phase)
Anterior-to-Posterior (AP)
Aligns with axial anatomy shape.
Slice Thickness
3 mm
Medium thickness for good resolution without sacrificing scan time or SNR.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
NEX / Averages
1–2 (1.5T)
1 (3T)
At 1.5T: 1-2 averages for good image quality.
At 3T: Single average sufficient due to signal gain.
Bandwidth
244 Hz/px (1.5T)
434 Hz/px (3T)
Matches frequency precession difference: ~220 Hz at 1.5T, ~440 Hz at 3T.
Turbo Factor / ETL
15–25
Optimized for selected echo time.
Saturation Band
On throat
Suppresses swallowing motion without covering region of interest.
Fold-over Suppression
Yes
Prevents wrap-around artifacts.
6. Planning Axial T1 TSE
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from the previous axial T2 sequence.
Keep the same slice angulation, coverage, and positioning to ensure images of different contrasts can be clearly compared.
Keep the same saturation band placement on the throat.
Parameter
Recommended Values
Why These Values
Echo Time (TE)
80–120 ms
Long TE required for T2 contrast.
Repetition Time (TR)
3,000–5,000 ms
Long TR required for T2 contrast.
Field-of-View (FOV)
160 × 140 mm
Reduced FOV aligns with axial anatomy shape.
Matrix
320 × 256 (1.5T) 260 × 224 (3T)
High matrix maintains consistent resolution for detailed axial assessment.
Foldover Direction (Phase)
Anterior-to-Posterior (AP)
Aligns with axial anatomy shape.
Slice Thickness
3 mm
Medium thickness for good resolution without sacrificing scan time or SNR.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
NEX / Averages
1–2 (1.5T)
1 (3T)
At 1.5T: 1-2 averages for good image quality.
At 3T: Single average sufficient due to signal gain.
Bandwidth
244 Hz/px (1.5T)
434 Hz/px (3T)
Matches frequency precession difference: ~220 Hz at 1.5T, ~440 Hz at 3T.
Turbo Factor / ETL
15–25
Optimized for selected echo time.
Saturation Band
On throat
Suppresses swallowing motion without covering region of interest.
Fold-over Suppression
Yes
Prevents wrap-around artifacts.
How to Avoid Artifacts When Planning the Sequences
The table below lists the 5 common cervical spine artifacts, and what techniques you can use to avoid them:
Artifacts
Solution – How to Avoid It
CSF flow artifacts
Set the fold-over direction foot-to-head to align with CSF flow direction.
Motion artifacts
Place saturation bands on the throat to reduce swallowing artifacts.
Wrap-around artifacts
Activate fold-over suppression to prevent anatomy outside the field of view from overlapping.
Chemical shift artifacts
Increase the bandwidth (220 Hz at 1.5T, 440 Hz at 3T).
Truncation artifacts
Increase the matrix size to capture more frequency information.
Part 3: Review the Images
Finally, we will review the images to ensure all the anatomical information we need is clear.
These key structures must be clearly visible in a cervical spine MRI:
Spinal cord and central canal
Cerebrospinal fluid spaces
Intervertebral discs (C2-C3 through C7-T1)
Vertebral bodies (C1-C7 and T1-T2)
Neural foramina and nerve roots
Ligamentous structures
Surrounding soft tissues
Below, we will go through all the different image contrasts and explain their specific role in imaging the cervical spine.
T2 TSE – Highlights Fluid-Related Tissues and Conditions
T2-weighted imaging makes fluids appear bright. This contrast is ideal for tissues and abnormalities with high water content.
In cervical spine MRI, T2 sequences are the gold standard for detecting spinal cord compression, disc herniation, myelopathy, and cord edema. The bright cerebrospinal fluid provides excellent contrast against the darker spinal cord, making compression visible as narrowing of the bright CSF space around the cord.
We capture T2 images in three planes (sagittal, coronal, and axial) to provide comprehensive visualization of spinal pathology from multiple angles.
✅ Sagittal T2 TSE of the Cervical Spine – Correct Image Example:
Things to Look for in Sagittal T2:
Bright CSF should surround the dark spinal cord without narrowing.
Intervertebral discs should show normal hydration (bright signal).
Look for disc herniations compressing the thecal sac.
Assess for cord signal changes indicating myelopathy.
✅ Coronal T2 TSE of the Cervical Spine – Correct Image Example:
Things to Look for in Coronal T2:
Neural foramina should be open and symmetric.
Look for lateral disc herniations or foraminal stenosis.
Assess spinal cord alignment and any lateral compression.
✅ Axial T2 TSE of the Cervical Spine – Correct Image Example:
Things to Look for in Axial T2:
Central canal should be patent with bright CSF.
Disc material should not indent the thecal sac.
Neural foramina should be symmetric and uncompressed.
Look for any soft tissue masses or ligamentum flavum hypertrophy.
STIR TSE – Clearest View of Fluid-Related Tissues and Conditions
STIR (Short Tau/TI Inversion Recovery) suppresses fat signals completely, which makes water-rich tissues stand out even clearer than with normal T2 TSE. This makes STIR ideal for detecting subtle fluid-related conditions – like edema, inflammation, and infections – where increased water content would otherwise be obscured by fat.
In the cervical spine, this contrast is particularly useful for identifying bone marrow edema, ligament tears, cord contusions, and infections like discitis or myelitis. STIR is crucial for detecting acute trauma injuries and inflammatory conditions where water content might not be visible on standard T2 sequences.
We capture STIR images in the sagittal plane to provide comprehensive assessment of inflammatory and traumatic changes.
✅ Sagittal STIR TSE of the Cervical Spine – Correct Image Example:
Things to Look for in Sagittal STIR:
Fat should appear uniformly dark (well-suppressed).
Look for bright signal in bones indicating marrow edema.
Assess ligaments for tears or inflammation.
Look for any inflammatory processes in soft tissues.
Evaluate for cord edema or contusion.
T1 TSE – Highlights Fat-Containing Tissues and Structural Abnormalities
T1-weighted imaging makes fat appear bright and fluid dark. This contrast is ideal for fat-rich tissues and structural abnormalities. T1 shows anatomical structures clearly, since it helps us see where different solid tissues like muscle and fat meet.
In cervical spine MRI, T1 sequences are important for evaluating vertebral body integrity, bone marrow pathology, and anatomical landmarks. T1 is also useful for detecting subacute hemorrhage, tumors, and serves as a baseline before contrast administration.
We capture T1 images in sagittal and axial planes to provide structural detail complementary to the T2 sequences.
✅ Sagittal T1 TSE of the Cervical Spine – Correct Image Example:
Things to Look for in Sagittal T1:
Vertebral bodies should show bright, uniform bone marrow signal.
Look for dark lesions indicating metastases or fractures.
Assess disc height and alignment.
Evaluate pre-vertebral soft tissues for masses or swelling.
✅ Axial T1 TSE of the Cervical Spine – Correct Image Example:
Things to Look for in Axial T1:
Bone marrow should appear bright and symmetric.
Look for fat-containing lesions like lipomas.
Assess vertebral body structural integrity.
Evaluate surrounding soft tissue anatomy.
Final Checks:
Before finishing a cervical spine MRI, always check these 5 points to ensure diagnostic quality:
Complete Coverage: All sequences must cover from the pons to T1-T2, including all seven cervical vertebrae and their discs.
Spinal Cord Visibility: The spinal cord and CSF spaces must be clearly visible throughout the cervical region in all sequences.
Image Quality: All images must have strong SNR, sharp anatomical detail, and no significant motion, flow, or chemical shift artifacts.
Consistent Planning: Sagittal, coronal, and axial planes must be properly aligned to the spinal anatomy for accurate assessment.
Artifact Management: Check that saturation bands are properly placed, fold-over suppression is active, and bandwidth is optimized for the field strength.



.avif)


.avif)
.avif)

.avif)