This step-by-step guide is for MRI students, radiographers, and technologists who wish to improve their planning skills and master the anal fistula MRI protocol.
What you will learn:
Key factors in anal fistula MRIs, including trade-offs.
Patient and scanner setup tips.
Best pulse sequences and planning techniques.
Ways to avoid common artifacts.
What great anal fistula images should look like.
Key Takeaways
Because anal fistula MRIs need to visualize tiny fluid-filled tracts, it's recommended to prioritize resolution.
The anal canal has complex, small structures where fistulas can form branching patterns. We need high resolution to detect these subtle tracts while keeping scan time short to avoid motion artifacts.
We typically 1) prioritize resolution, 2) maintain short scan time, and 3) optimize SNR as needed.
We mainly use T2 TSE sequences with fat saturation in anal fistula MRIs.
T2 sequences make fluid appear bright, helping us see fistula tracts clearly against darker tissue. Fat saturation enhances this contrast by suppressing the bright fat signal.
This makes inflamed tissue and fluid collections stand out more.
Avoid these 5 common anal fistula artifacts.
Artifacts
Solution – How to Avoid It
Motion artifacts
Shorten scan time using parallel imaging or radial k-space acquisition (BLADE/PROPELLER).
Susceptibility artifacts
Use turbo spin echo instead of gradient echo sequences to reduce sensitivity to gas interfaces.
Wrap-around artifacts
Activate fold-over suppression to prevent anatomy outside the field of view from overlapping.
Chemical shift artifacts
Increase the bandwidth to reduce the spatial displacement between fat and water signals.
Fat suppression failure
Use STIR instead of spectral fat saturation when field inhomogeneity is present.
Intro to Anal Fistula MRIs
The anal canal and surrounding perianal region are complex anatomical areas where abnormal connections called fistulas can develop between the anal canal and the skin surface. These tracts often result from infection, inflammation, or surgical complications.
Anal fistula MRI is one of the most important pelvic imaging protocols for colorectal surgery planning. It provides detailed visualization of fistula tracts, their relationship to sphincter muscles, and any associated abscesses or inflammation.
How to Balance the 3 Trade-offs in Anal Fistula MRIs
In MRI, we always face a trade-off between 3 key metrics:
Scan Time: How fast a pulse sequence can be completed.
Resolution: How much detail the image can display.
SNR: How clear the image is, how much signal relative to noise.
Improving one of these metrics reduces the performance of the others. To decide what trade-offs to make, we must consider the needs of each clinical situation.
In anal fistula MRIs, we need to visualize tiny fluid-filled tracts in soft tissue. The pelvic region is also subject to bowel movement and other motion. Small or branching fistulas require exceptional detail to plan surgery properly.
Therefore, we typically 1) prioritize resolution, 2) maintain short scan time to reduce motion artifacts, and 3) optimize SNR as needed for clear tissue contrast.
Note! Prioritizing resolution in anal fistula MRIs is only a general guideline, NOT a strict rule. If your patient has difficulty staying still or the bowel motion is excessive, you may need to prioritize scan time instead. The right balance always depends on the needs of your patient and clinic.
Anal Fistula Health Conditions and the MRI Sequences That Reveal Them
The anal fistula MRI study helps us diagnose and characterize various perianal conditions. The table below lists the most common conditions and the pulse sequences that reveal them:
Makes fluid appear bright against darker tissue, clearly showing tubular fistula tracts. Simple fistulas run straight from internal to external sphincter, while complex ones branch or take indirect paths.
Suppresses fat to highlight fluid collections and inflamed tissue. The increased contrast-to-noise ratio between normal fat and abnormal fluid makes even small abscesses visible. Critical for identifying hidden pockets of infection.
Nulls fat signal completely while highlighting all water content in tissues. Shows the full extent of edema and inflammatory spread. Detects inflammation based on increased water content, whether acute or chronic. Most sensitive for mapping inflammatory extent.
Highlights fat and provides clear anatomical contrast. Shows structural details and chronic changes. Provides baseline anatomy before contrast administration.
Active disease and viability:
• Abscess walls (rim enhancement)
• Active granulation tissue
• Tumor involvement
• Fistula tract viability
T1 TSE (Post-contrast)
Shows tissues with active blood supply through enhancement. Granulation tissue enhances, fibrosis does not. Abscess walls show rim enhancement. Critical for differentiating healing tissue from scar.
How to Perform an Anal Fistula MRI Protocol
The step-by-step guide below will show you how to set up and perform an anal fistula MRI protocol in practice.
We will perform the protocol in 3 parts:
Set up the Patient and MRI Scanner
Plan and Acquire the Protocol Sequences
Review the Images
Part 1: Set up the Patient and MRI Scanner
1. Prepare the Patient
Before scanning, proper patient preparation is crucial for optimal image quality.
The patient should empty their bladder before the exam. A full bladder can deform rectal anatomy and create interfaces between fluid and gas that impair fat suppression.
Ask the patient to avoid gas-producing foods like fiber for 24 hours before the scan if possible. Excessive bowel gas creates susceptibility artifacts and degrades image quality.
Some protocols may require a small rectal enema to clear feces from the rectum, but this is institution-specific.
2. Position the Patient in the Scanner
Lay the patient feet-first and supine (on their back) with the pelvis centered at the scanner's isocenter.
Using a feet-first position makes the scan feel less claustrophobic for the patient, which reduces the risk of motion artifacts.
Use a pelvic phased-array coil or body coil to ensure high-resolution imaging. Position the coil's upper border at the iliac crest. This coil provides strong signal reception and full coverage of the perianal region.
✅ Correct Patient Positioning:
3. Check the Scanner’s Hardware Settings
Once the patient is in place, review your scanner’s hardware settings.
In this guide, we will use the following settings:
Scanner Setting
Value
Why This Value
Magnetic field strength
1.5 T
Enables high Signal-to-Noise Ratio, which gives superior image quality.
Maximum gradient strength
45 mT/m
Enables faster acquisitions while preserving high image quality.
This hardware setup is widely used in clinical practice. It balances acquisition time, image quality, and patient comfort.
4. Capture the Initial Localizer Images
Before we can perform any MRI protocol, we must always capture initial localizer images of the patient. These images act as a guide for planning the detailed scans we will perform next.
We should always capture localizers in three planes:
Axial
Sagittal
Coronal
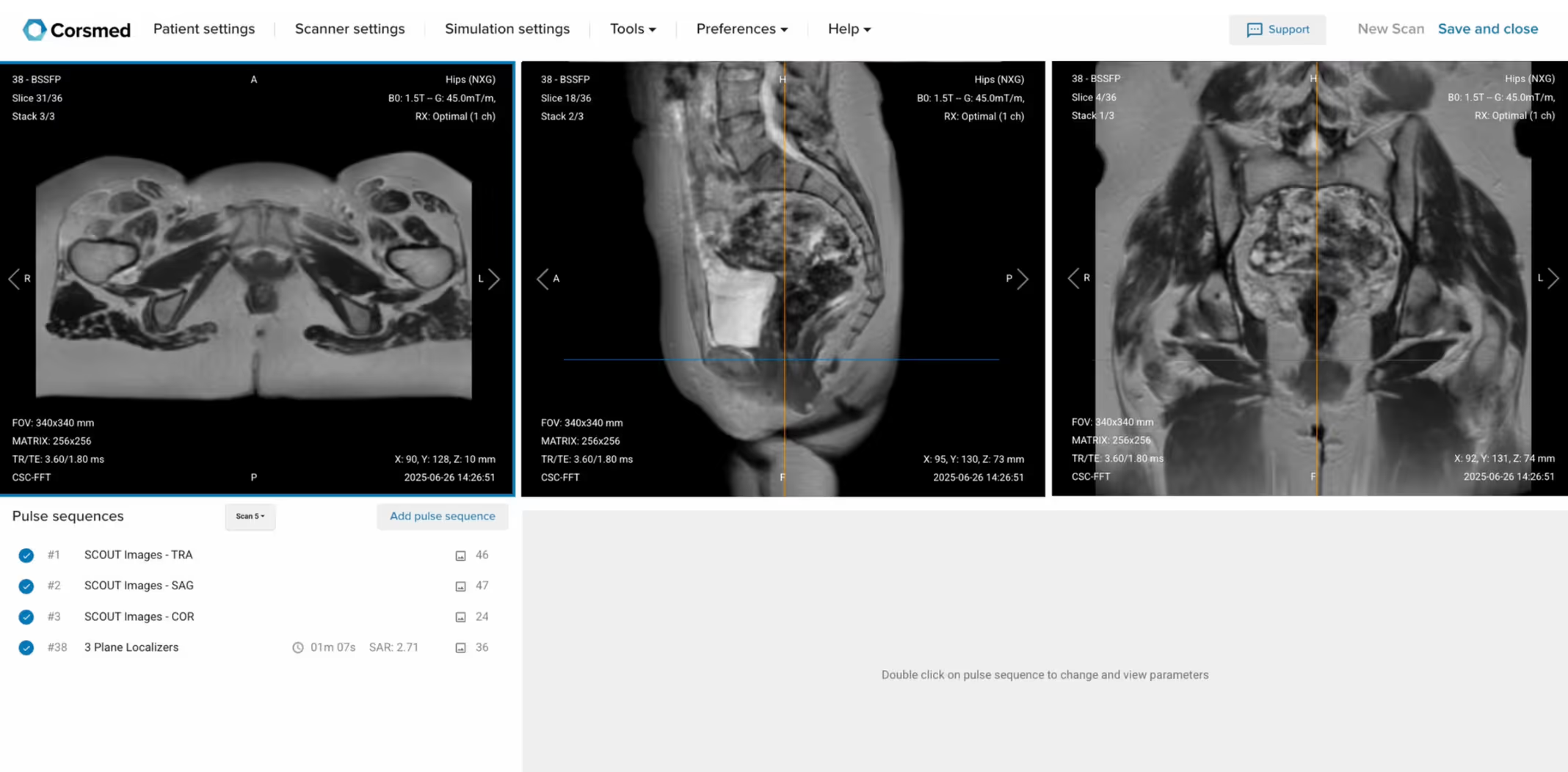
Once acquired, upload the initial localizer images into the three viewports.
Then, scroll through each of the image stacks to locate a central slice that clearly shows the anatomy of the anal canal.
✅ Correct Setup of Localizer Images for Anal Fistula MRI:
Part 2: Plan and Acquire the Protocol Sequences
When all preparations are ready, we can start planning and acquiring the protocol sequences.
Let's go through the pulse sequences a standard anal fistula MRI protocol includes, why we perform them, and how to set them up.
The 6 Sequences of a Standard Anal Fistula MRI Protocol
Sagittal T2 TSE High Resolution
Sagittal T2 TSE Fat-Saturated (SPAIR or STIR)
Axial T2 TSE Fat-Saturated (SPAIR or STIR)
Coronal T2 TSE Fat-Saturated (SPAIR or STIR)
Sagittal T1 TSE (Pre-contrast)
Sagittal T1 TSE (Post-contrast)
We mainly use T2 Turbo Spin Echo sequences with fat saturation for this study. These sequences make fluid appear bright, which helps us detect fistula tracts, abscesses, and inflammation clearly against darker tissue.
Fat saturation techniques enhance this contrast further by suppressing the bright fat signal. This increases the contrast-to-noise ratio between pathology and normal tissue.
In the sections below, we go through how to plan and set up each sequence.
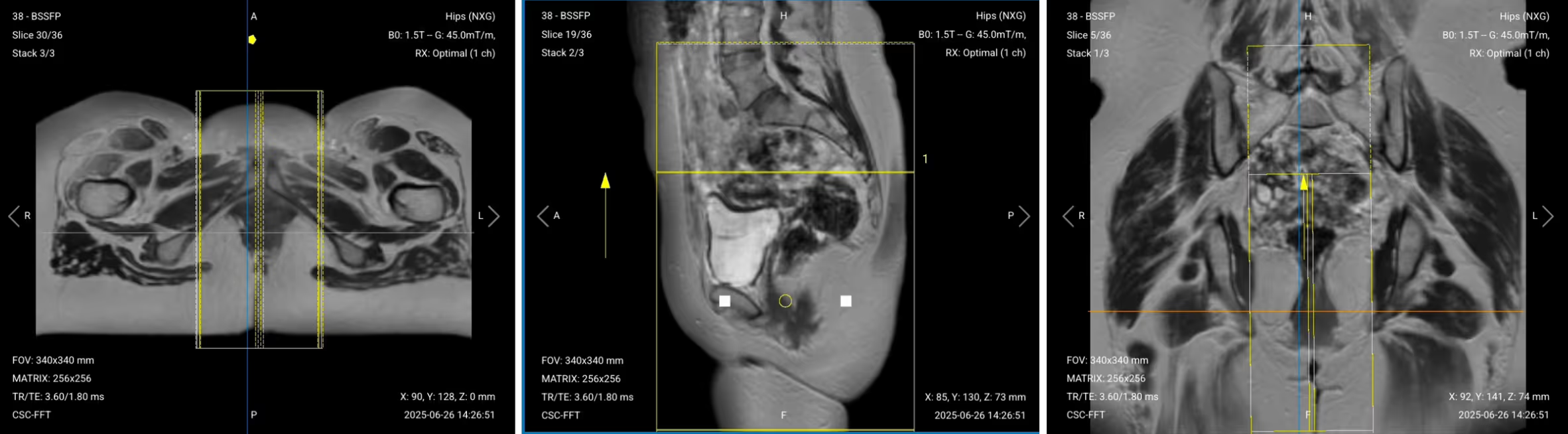
1. Sagittal T2 TSE High Resolution
✅ Correct Planning:
Planning Instructions:
Use the anal canal and rectum as your anatomical references.
Align the slices as follows:
Axial localizer: Position slices through the midline of the anal canal.
Coronal localizer: Angle slices to be exactly in the middle of the rectum, following its axis.
Use appropriate geometry parameters:
Slice number: 15–20 to fully cover the perianal region.
Slice thickness: 3 mm for high resolution without sacrificing SNR.
Slice gap: 0.3 mm (10% of thickness) to prevent crosstalk while maintaining continuity.
Set the fold-over direction (phase encoding) to foot–head (FH) to reduce wrap and respiratory motion artifacts.
Ensure coverage from the buttock cheek posteriorly to the upper rectum anteriorly.
Parameters for Sagittal T2 TSE High Resolution:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
90–110 ms
Longer TE required for T2 contrast to highlight fluid.
Repetition Time (TR)
3,000–4,000 ms
Longer TR required for T2 contrast.
Field-of-View (FOV)
200 × 200 mm
Small enough to focus on the perianal region with high detail.
Matrix
320 × 320
High matrix for excellent resolution to detect small fistula tracts.
Foldover Direction (Phase)
Foot-to-Head (FH)
Reduces respiratory motion and wrap artifacts.
Number of Slices
15–20
Enough to cover the entire perianal region and lower rectum.
Slice Thickness
3 mm
Thin slices for high resolution without losing too much SNR.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
NEX / Averages
2
Higher averages improve SNR for better visualization of small structures.
Turbo Factor / ETL
15–18
High turbo factor for faster scanning while maintaining T2 contrast.
Bandwidth
150–200 Hz/px
Medium bandwidth balances chemical shift reduction with SNR preservation.
Fold-over Suppression
Yes
Prevents wrap-around artifacts from adjacent anatomy.
Choosing Fat Suppression for Anal Fistula MRI: SPAIR vs STIR
The following T2 sequences will use fat suppression.
When imaging anal fistulas, however, it’s very important to select the right fat suppression technique for image quality.
There are two main fat suppression options:
SPAIR (Spectral Fat Saturation):SPAIR uses a specific pulse to suppress fat based on its frequency. It's faster than STIR and provides more robust suppression when the magnetic field is uniform.
However, SPAIR is very sensitive to field inhomogeneity. In the pelvis, interfaces between water (bladder), gas (bowel), and tissue create field variations that can cause SPAIR to fail.
STIR (Inversion Recovery):STIR works by setting an inversion time that nulls fat signal completely. It's less sensitive to field inhomogeneity, making it more reliable when bowel gas or poor patient preparation creates field distortions.
Which to Choose for Anal Fistula MRI:
First choice: SPAIR when the patient is well-prepared (empty bladder, minimal bowel gas)
The typical inversion time for STIR at 1.5T is 150-180 milliseconds. While STIR takes longer than SPAIR, its robust suppression often makes it worth the extra time in pelvic imaging.
2. Sagittal T2 TSE Fat-Saturated (SPAIR or STIR)
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from the previous Sagittal T2 TSE sequence.
Keep the same slice angulation, coverage, and positioning to ensure images of different contrasts can be clearly compared.
Parameters for Sagittal T2 TSE Fat-Saturated:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
90–110 ms
Longer TE required for T2 contrast to highlight fluid.
Repetition Time (TR)
3,000–4,000 ms
Longer TR required for T2 contrast.
Inversion Time (TI)
150–180 ms (for STIR)
Nulls fat signal at 1.5T for robust suppression.
Field-of-View (FOV)
200 × 200 mm
Small enough to focus on the perianal region with high detail.
Matrix
320 × 320
High matrix for excellent resolution to detect small fistula tracts.
Foldover Direction (Phase)
Foot-to-Head (FH)
Reduces respiratory motion and wrap artifacts.
Number of Slices
15–20
Enough to cover the entire perianal region and lower rectum.
Slice Thickness
3 mm
Thin slices for high resolution without losing too much SNR.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) prevents crosstalk while maintaining continuity.
NEX / Averages
2
Higher averages improve SNR for better visualization of small structures.
Turbo Factor / ETL
15–18
High turbo factor for faster scanning while maintaining T2 contrast.
Bandwidth
150–200 Hz/px
Medium bandwidth balances chemical shift reduction with SNR preservation.
Fat Suppression
STIR or SPAIR
STIR more robust for inhomogeneous fields; SPAIR faster if field is uniform.
Fold-over Suppression
Yes
Prevents wrap-around artifacts from adjacent anatomy.
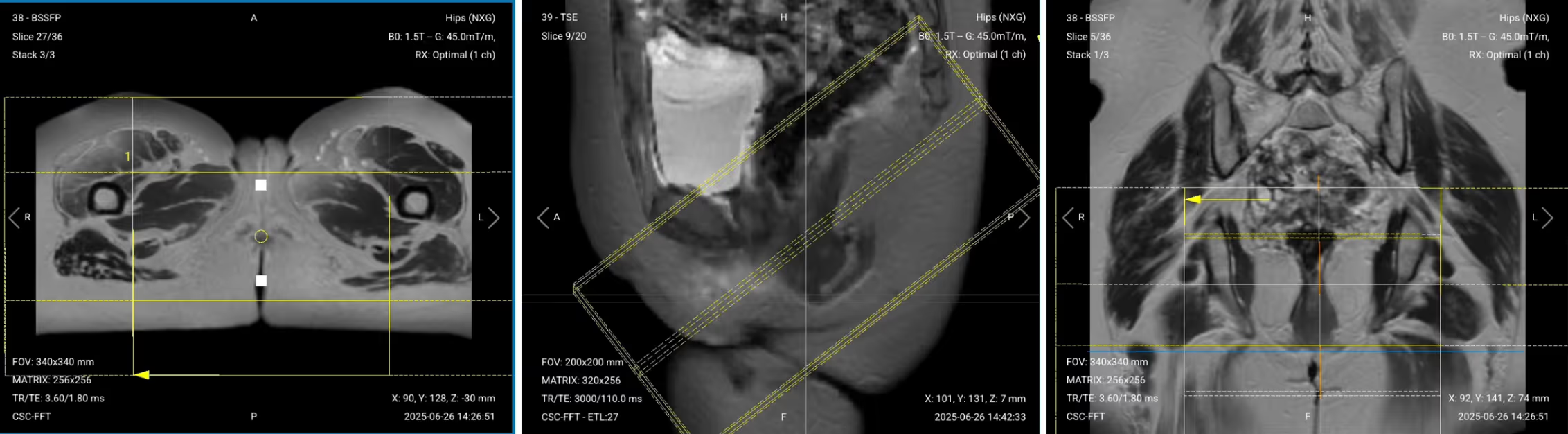
3. Axial PD Fat-Saturated TSE (SPAIR or STIR)
✅ Correct Planning:
Planning Instructions:
Use the anal canal and internal anal sphincter as your anatomical references.
Align the slices as follows:
Sagittal localizer: Position slices perpendicular to the anal canal axis.
Coronal localizer: Ensure slices are perpendicular to the anal canal.
Use appropriate geometry parameters:
Slice number: 20–25 to cover from above the levator ani to the perineal skin.
Slice thickness: 3–4 mm for good resolution while maintaining SNR.
Slice gap: 0.3–0.4 mm (10% of thickness) to avoid missing pathology.
Set the fold-over direction (phase encoding) to right–left (RL) to reduce motion artifacts from bowel.
Parameters for Axial T2 TSE Fat-Saturated:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
90–110 ms
Longer TE required for T2 contrast to highlight fluid.
Repetition Time (TR)
3,000–4,000 ms
Longer TR required for T2 contrast.
Inversion Time (TI)
150–180 ms (for STIR)
Nulls fat signal at 1.5T for robust suppression.
Field-of-View (FOV)
180 × 180 mm
Small FOV for high resolution of the perianal region.
Matrix
256 × 256
High matrix provides detailed visualization of sphincter anatomy.
Foldover Direction (Phase)
Right-to-Left (RL)
Reduces bowel motion artifacts and phase wrap.
Number of Slices
20–25
Covers from levator ani to perineal skin.
Slice Thickness
3–4 mm
Medium thickness balances resolution and SNR.
Slice Gap
0.3–0.4 mm
Minimal gap (10% of thickness) ensures complete coverage.
NEX / Averages
2
Higher averages improve SNR for small structure visualization.
Turbo Factor / ETL
15–18
High turbo factor for faster scanning while maintaining T2 contrast.
Bandwidth
150–200 Hz/px
Medium bandwidth balances chemical shift reduction with SNR.
Fat Suppression
STIR
More robust than SPAIR when field inhomogeneity is present.
Fold-over Suppression
Yes
Prevents wrap-around artifacts from pelvic structures.
4. Coronal T2 TSE Fat-Saturated (SPAIR or STIR)
✅ Correct Planning:
Planning Instructions:
Use the anal canal as your anatomical reference.
Align the slices as follows:
Sagittal localizer: Position slices parallel to the anal canal axis.
Axial localizer: Ensure coverage of the ischiorectal fossae bilaterally.
Use appropriate geometry parameters:
Slice number: 15–20 to cover from rectum posteriorly to pubic symphysis anteriorly.
Slice thickness: 3–4 mm for adequate resolution.
Slice gap: 0.3–0.4 mm (10% of thickness) to maintain continuity.
Set the fold-over direction (phase encoding) to right–left (RL) to minimize motion artifacts.
Ensure coverage includes horseshoe tracts and bilateral ischiorectal fossae.
Parameters for Coronal T2 TSE Fat-Saturated:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
90–110 ms
Longer TE required for T2 contrast to highlight fluid.
Repetition Time (TR)
3,000–4,000 ms
Longer TR required for T2 contrast.
Inversion Time (TI)
150–180 ms (for STIR)
Nulls fat signal at 1.5T for robust suppression.
Field-of-View (FOV)
200 × 200 mm
Wide enough to include bilateral ischiorectal fossae.
Matrix
256 × 256
High matrix for detailed anatomical visualization.
Foldover Direction (Phase)
Right-to-Left (RL)
Reduces motion artifacts from bowel and breathing.
Number of Slices
15–20
Covers from posterior rectum to anterior pubis.
Slice Thickness
3–4 mm
Medium thickness balances resolution and SNR.
Slice Gap
0.3–0.4 mm
Minimal gap (10% of thickness) ensures complete coverage.
NEX / Averages
2
Higher averages improve SNR for pathology detection.
Turbo Factor / ETL
15–18
High turbo factor for efficient T2 contrast acquisition.
Bandwidth
150–200 Hz/px
Medium bandwidth reduces chemical shift while preserving SNR.
Fat Suppression
STIR
Robust suppression despite field inhomogeneity from gas.
Fold-over Suppression
Yes
Prevents aliasing from lateral pelvic structures.
5. Sagittal T1 TSE (Pre-contrast)
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from the previous Sagittal T2 TSE sequence.
Keep the same slice angulation, coverage, and positioning to ensure images of different contrasts can be clearly compared.
Parameters for Sagittal T1 TSE (Pre-contrast):
Parameter
Recommended Values
Why These Values
Echo Time (TE)
10–15 ms
Short TE required for T1 contrast.
Repetition Time (TR)
400–600 ms
Short TR required for T1 contrast.
Field-of-View (FOV)
200 × 200 mm
Matches T2 sequences for comparison.
Matrix
256 × 256
Medium-high matrix for good anatomical detail.
Foldover Direction (Phase)
Foot-to-Head (FH)
Consistent with other sagittal sequences.
Number of Slices
15–20
Matches coverage of T2 sequences.
Slice Thickness
3 mm
Thin slices for detailed anatomy.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) for continuity.
NEX / Averages
1–2
Standard averaging for T1 contrast.
Turbo Factor / ETL
3–5
Low turbo factor preserves T1 contrast.
Bandwidth
150–200 Hz/px
Medium bandwidth for balanced SNR and artifact reduction.
Fold-over Suppression
Yes
Prevents wrap artifacts.
Parallel Imaging
Optional (GRAPPA 2)
Reduces scan time if multi-channel coil available.
6. Sagittal T1 TSE (Post-contrast)
After administering gadolinium contrast (typically 0.1 mmol/kg body weight), wait approximately 30-60 seconds before acquiring post-contrast images.
✅ Correct Planning:
Planning Instructions:
Copy the slice geometry and planning from the previous pre-contrast T1 TSE sequence.
Keep the same slice angulation, coverage, and positioning to ensure precise comparison between pre- and post-contrast images.
Consider adding fat saturation to post-contrast T1 for better visualization of enhancing tissue.
Parameters for Sagittal T1 TSE Post-contrast:
Parameter
Recommended Values
Why These Values
Echo Time (TE)
10–15 ms
Short TE required for T1 contrast.
Repetition Time (TR)
400–600 ms
Short TR required for T1 contrast.
Field-of-View (FOV)
200 × 200 mm
Matches pre-contrast for direct comparison.
Matrix
256 × 256
Medium-high matrix for good anatomical detail.
Foldover Direction (Phase)
Foot-to-Head (FH)
Consistent with pre-contrast sequence.
Number of Slices
15–20
Matches pre-contrast coverage exactly.
Slice Thickness
3 mm
Same as pre-contrast for comparison.
Slice Gap
0.3 mm
Minimal gap (10% of thickness) for continuity.
NEX / Averages
1–2
Standard averaging for T1 contrast.
Turbo Factor / ETL
3–5
Low turbo factor preserves T1 contrast.
Bandwidth
150–200 Hz/px
Medium bandwidth for balanced SNR and artifact reduction.
Fat Suppression
Optional (Spectral)
Improves visualization of enhancing tissue by suppressing fat.
Fold-over Suppression
Yes
Prevents wrap artifacts.
Parallel Imaging
Optional (GRAPPA 2)
Reduces scan time if multi-channel coil available.
How to Avoid Artifacts When Planning the Sequences
The table below lists the 5 common anal fistula artifacts, and what techniques you can use to avoid them:
Artifacts
Solution – How to Avoid It
Motion artifacts
Shorten scan time using parallel imaging or radial k-space acquisition (BLADE/PROPELLER).
Susceptibility artifacts
Use turbo spin echo instead of gradient echo sequences to reduce sensitivity to gas interfaces.
Wrap-around artifacts
Activate fold-over suppression to prevent anatomy outside the field of view from overlapping.
Chemical shift artifacts
Increase the bandwidth to reduce the spatial displacement between fat and water signals.
Fat suppression failure
Use STIR instead of spectral fat saturation when field inhomogeneity is present.
Part 3: Review the Images
Finally, we will review the images to ensure all the anatomical information we need is clear.
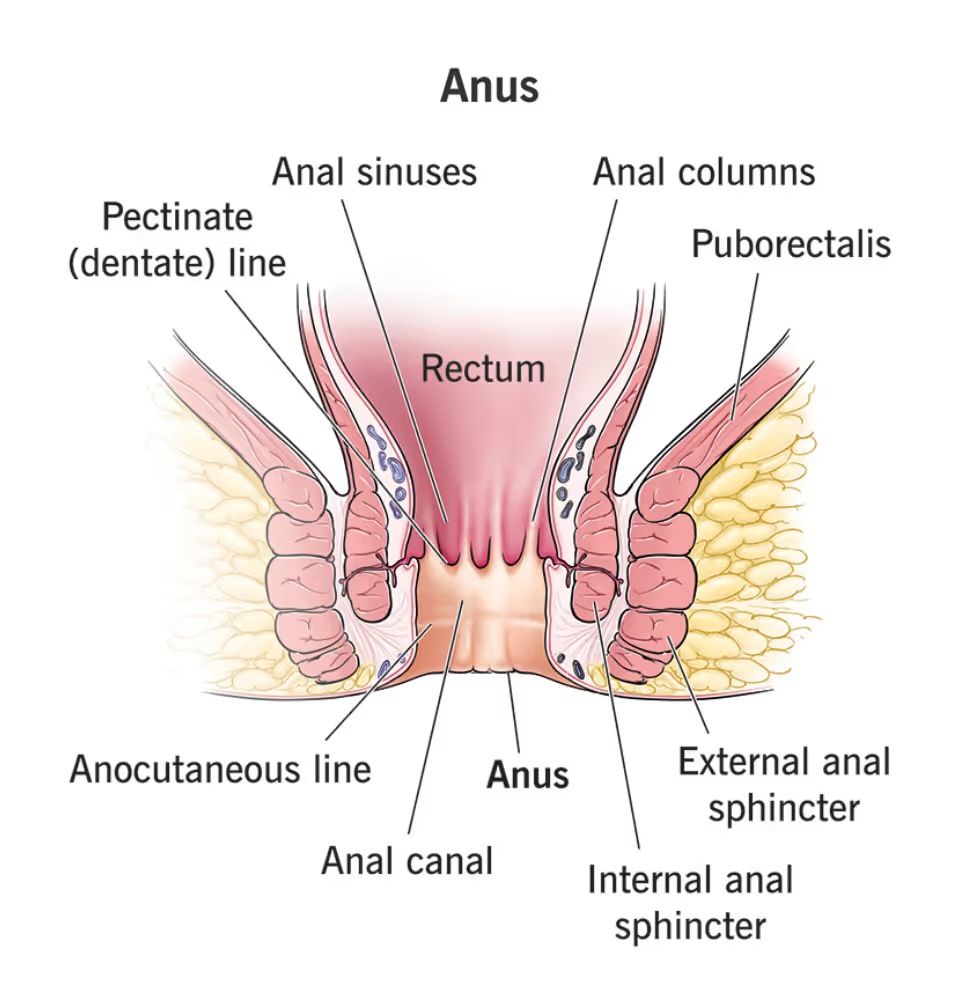
These key structures must be clearly visible in an anal fistula MRI:
Internal and external anal sphincters
Levator ani muscle
Ischiorectal fossae
Perianal skin and subcutaneous tissue
Rectum and anal canal
Any fistula tracts, abscesses, or inflammatory changes
Below, we will go through all the different image contrasts and explain their specific role in imaging anal fistulas.
T2 TSE – Highlights Fluid-Filled Tracts and Anatomy
T2-weighted imaging makes fluids appear bright. This contrast is ideal for tissues and abnormalities with high water content.
In anal fistula MRI, T2 sequences are the workhorse for detecting fistula tracts, which appear as bright tubular structures against darker muscle and fat. They help us map the exact course of fistulas through the sphincter complex and identify branching patterns.
We acquire sagittal views to assess the relationship between fistulas and the rectum, and to understand anterior-posterior spread.
T2 Fat-Saturated – Mapping Inflammatory Extent Through Edema
T2 Fat-Saturated imaging suppresses fat while keeping fluid bright. This shows all areas with increased water content, making it the most sensitive sequence for detecting inflammatory spread.
In anal fistula MRI, STIR reveals the full extent of inflammation by highlighting edema in tissues. Any area with increased water appears bright, whether from acute infection or chronic inflammation. This complete map of inflammatory spread helps surgeons plan their approach.
We acquire fat-saturated T2 in all three planes to fully understand the fistula's path and extent:
Sagittal views show the vertical relationship to the rectum and sphincters.
Axial views best demonstrate tracts crossing from internal to external sphincter.
Coronal views reveal horseshoe extensions and bilateral spread that might be missed in other planes.
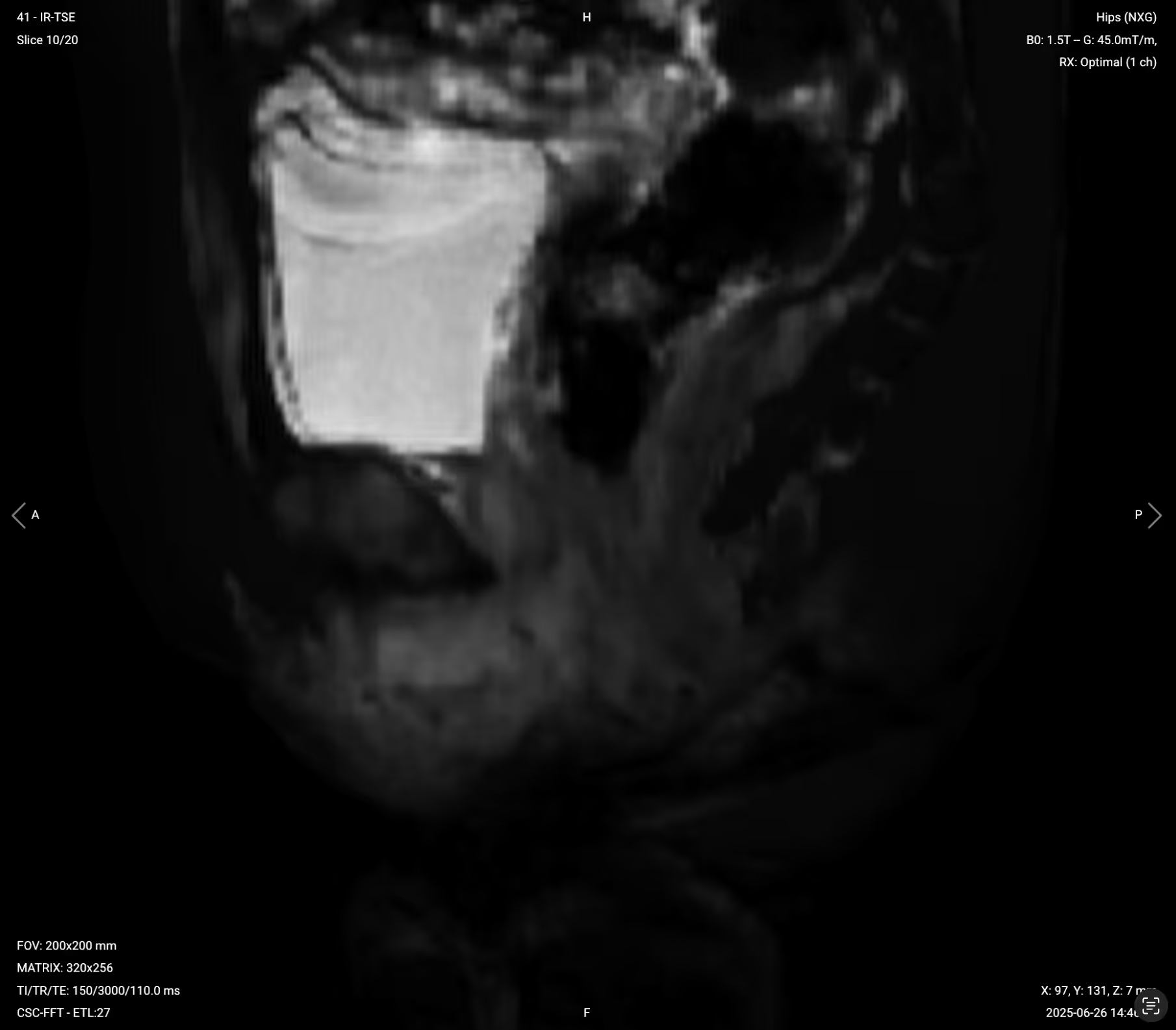
❌ Failed Spectral Fat Saturation (SPAIR) – Example of Poor Suppression:
Signs of Failed Fat Suppression:
Heterogeneous fat signal (some areas bright, others dark)
Relationship between fistula and sphincter complex
Vertical extent of inflammatory changes
We then acquire axial views perpendicular to the anal canal for the most diagnostic images, as they show tracts crossing from internal to external sphincter clearly.
T1 TSE Pre-contrast – Structural Detail and Chronic Changes
T1-weighted imaging makes fat appear bright and fluid dark. This contrast is ideal for fat-rich tissues and structural abnormalities. T1 shows anatomical structures clearly, since it helps us see where different solid tissues like muscle and fat meet.
In anal fistula MRI, pre-contrast T1 sequences provide baseline anatomy and help identify chronic fibrotic changes. They show the normal fat planes between muscles and help detect fat infiltration or obliteration that indicates chronic inflammation.
We acquire pre-contrast T1 in the sagittal plane to match our T2 sequences for direct comparison.
Fat planes between muscles preserved or obliterated
Chronic fibrotic changes (intermediate signal)
Baseline anatomy before contrast enhancement
T1 TSE Post-contrast – Identifying Viable Tissue Through Enhancement
Post-contrast T1 shows where gadolinium accumulates in tissues with active blood supply and leaky vessels. Enhancement indicates viable, vascularized tissue.
In anal fistula MRI, post-contrast T1 differentiates healing tissue from mature scar. Active granulation tissue in fistula walls enhances brightly, while chronic fibrotic tracts show little to no enhancement. Abscesses show characteristic rim enhancement around a dark center of pus.
These contrasts help surgeons identify which tissue can heal versus what needs removal.
We typically acquire post-contrast T1 in the same sagittal plane as pre-contrast for direct comparison. Some protocols may add axial or coronal post-contrast sequences for complex cases.






%20Fat%20Saturation%2C%20Failed.avif)